Abstract
This report introduces a simple and feasible questionnaire that attempts to explore the awareness and knowledge of consumers regarding some basic concepts on diet and health. The questions were designed to examine consumers’ general health concern and self-perceived health status, basic knowledge about metabolic disorders, how diet influences health, and knowledge and consumption of Functional Foods and Nutraceuticals. They were additionally inquired about their awareness of the inter-individual differences in response to diet. The survey revealed that the interviewed consumers subpopulation (N=253 Spanish participants) had good metabolic health and healthy lifestyle habits. Despite their concern about health and, awareness of the relevance of diet to health, their familiarity with chronic metabolic disorders or novel foods such as Functional Foods and Nutraceuticals was limited but they manifested interest in learning more about these issues. The concept of inter-individual variability in response to diet was familiar to some but generally poorly understood.
Keywords
Self-perceived health status; lifestyle habits; healthy diet; metabolic disorders; functional foods; nutraceuticals; questionnaire; inter-individual differences.
Introduction
An important wellbeing promoting strategy in westernized countries is the encouragement of a healthy life-style, including improved eating habits, as a means to prevent the development of metabolic chronic disorders associated with sedentariness and increased consumption of high-energy foods. In Spain, despite general efforts on the dissemination of information about healthy habits, the prevalence of some chronic non-communicable metabolic diseases: obesity [1], hypercholesterolemia [2], hypertension [3], type-2 diabetes [4] or metabolic syndrome (MetS) [5] remains high and constitutes a major medical and economy burden. It has been indicated that the incidence of these disorders is strongly associated with the individuals’ health behavior. In general, consumers with higher levels of health motivation and consciousness as well as greater knowledge of health and disease issues will exhibit greater levels of preventive health behaviors [6]. Nevertheless, adopting these behaviors is a complex process affected by different factors and thus, discrepancies may occur between an individual’s health perception, their true health status and the adoption of healthy habits.
It has been shown that awareness of cardio-metabolic risk factors is low in high-risk populations [7]. Consumers with unhealthy habits (smoking, sedentariness) may not perceive themselves as unhealthy since they may not be aware of the presence of these so-called ‘silent disorders’ such as hypercholesterolemia or hypertension and thus they are not inclined to adopt a healthier lifestyle [8, 9]. In a Polish study, 91% of patients with diagnosed MetS led a sedentary lifestyle and none followed cardio-protective diet recommendations [10]. Besides, an American study suggested that consumers diagnosed with both high cholesterol and hypertension, were the greatest users of nutrient information from the Nutrition Fact Panel [11], however, they did not find if their choice was affected by the nutritional information given. The lack of information about metabolic diseases can contribute to limit the adoption of healthier recommendations and thus, an increase in the awareness and knowledge of cardio-metabolic risk associated factors are believed to be significant for adopting healthy lifestyle behaviors.
Moreover, adopting healthy eating habits is one of the most important and commonly reported reasons for successful prevention of metabolic disorders. A general knowledge of a healthy diet is associated, to a certain extent, with an understanding of the overall recommendations for the consumption of a diversity of foods: vegetables and fruits, fats, olive oil, cereals, salt, refined and processed foods, meat [12–14]. Enhancing the level of awareness of the role of diet in health will influence individual’s food choices and quality and, consequently, the adoption of healthier eating habits [15].
In addition to the dietary recommendations, two new categories of foods and food products entered the healthy eating market some time ago: Functional Foods and Nutraceuticals. These food items are designed to contain a component or components scientifically linked with a health benefit beyond nutrition [16], and to help in the fight against the development of chronic diet-related disorders such as hypertension, hypercholesterolemia, type-2 diabetes and other inflammatory oxidative processes [17]. Functional Foods are foods that can be consumed as part of the usual diet (e.g. margarine enriched with cholesterol-lowering plant sterols) whereas Nutraceuticals are concentrated food extracts consumed as a pill, capsule or powder supplementary to the diet [18]. Several factors would influence the consumer acceptance of Functional Foods: knowledge or awareness of the concept, necessity, perceived reward, confidence or belief in the health benefits, taste or quality [19–21]. Knowledge and understanding of Nutraceuticals appear to be rather limited even in highly specialized subpopulations such as pharmacist students [22]. Increasing the knowledge and understanding of these products is important for their successful marketing and it might also contribute to reinforcing the adoption of behavioral changes towards a healthier eating.
It is conceivable that the perception by the Spanish consumers of the diet-related metabolic disorders and of the feasibility of their prevention by healthier behaviors remains insufficient [3, 5, 23]. Whether the general population has yet become fully aware of the relevance of adopting healthy dietary habits for the prevention of chronic metabolic diseases, has started applying these habits and has truly understood why they should do it, constitute critical points for the successful implementation of dietary and lifestyle recommendations to reduce the burden of these diseases. Nutritional awareness seems to remain low among the general public and understanding of dietary information remains difficult for many people [24]. Therefore, there is an emerging use of short and simple dietary questionnaires to investigate the association between healthy-eating attitudes and the development of chronic diseases. These questionnaires may be a useful tool for the prevention of these diseases [25].
All things considered, the aim of this pilot study was to attain a preliminary simple questionnaire designed to have an overview of people´s awareness and understanding of some basic issues in relation to diet and health in a Spanish subpopulation that will help in the future to develop health preventing programs. For this purpose we prepared a feasible and comprehensive simple questionnaire divided into 22 items that aimed at specifically assessing: i) self-perceived overall health status and health concern, ii) general knowledge about some highly prevalent chronic metabolic disorders, iii) perception of the influence of diet in health, and iv) awareness and consumption of Functional Foods and Nutraceuticals. In addition, we made an initial attempt to find out whether the participants had any understanding of potential differences in the effects of diet and food in different individuals. A last question of the survey was posed to identify the attitude of the participants about research in the area of food and health.
Methodology
Demographic Characteristics of the Participants and Anthropometric Measurements
Consumers were recruited during a science event (The week of Science) carried out in Spain at two separate places: CIAL-CSIC in Madrid and CEBAS-CSIC in Murcia, respectively. Finally, a total of 253 random attendants took part in the study: 123 participants (48.6%) in Madrid and 130 participants (51.4%) in Murcia. Distribution of the total sample population by the location, gender and age group (adolescents [11 to 17 years old], young adults [18 to 40 years old] and adults [41 to 65 years old]) is displayed in Table 1. The group was constituted by a 59.3% of women and a 40.7% of men with slightly higher proportion of young adults (40.3%) and, in particular of young adult women (46.7%). During the face-to-face interview, the participants were weighed (kg) using a digital weight scale (Medisana AG, Germany) and their height measured (cm) in erect position and bare feet with a portable stadiometer allowing standing-height measurement in metric values (Seca, Handover, Germany). These values were used to calculate the body mass index (BMI). We also measured their waist circumference (WC, cm) and hip circumference (cm) and calculated the waist-to-hip ratio (WHR). Systolic and diastolic blood pressure (SBP, DBP; mm Hg) were estimated using an automatic upper arm blood pressure monitor MTS (Medisana AG, Germany). The volunteers were allowed to sit down and relax for a few minutes before the monitoring. We additionally assessed their smoking, alcohol drinking and sport practicing habits. Each volunteer was given an alphanumeric code for identification and collected data were coded and processed anonymously.
Table 1. Socio-demographic characteristics of the sample population: distribution by location, gender and age group.
|
Characteristics |
Total n (%) |
Men n (%) |
Women n (%) |
|
Location |
|||
|
Murcia |
130 (51.4) |
49 (47.6) |
81 (54.0) |
|
Madrid |
123 (48.6) |
54 (52.4) |
69 (46.0) |
|
Total |
253 (100) |
103 (40.7) |
150 (59.3) |
|
Age group |
|
|
|
|
Adolescents [11–17 y] |
82 (32.4) |
36 (35.0) |
46 (30.7) |
|
Young adults [18–40 y] |
102 (40.3) |
32 (31.1) |
70 (46.7) |
|
Adults [41–65 y] |
69 (27.3) |
35(34.0) |
34 (22.7) |
n= number of participants.
Questionnaire
Volunteers were asked to complete a self-administered questionnaire developed by the researchers involved in this project (Supplementary Material S1). The questionnaire was composed of 22 items divided into several sections. In the first section (items 1 to 6), participants were asked about their concern and perception of their health status and about their general knowledge on several metabolic chronic disorders (hypercholesterolemia, hypertension, type-2 diabetes and metabolic syndrome). In the second part of the survey, the participants were asked a series of knowledge and awareness questions regarding the association between food/diet and health (items 7 to 10). The third section (items 11 to 20) focused on new food and derived products with healthy effects: Functional Foods and Nutraceuticals and aimed at finding whether the participants had any knowledge of these products and whether they consumed or would consume them. Question 21 was focused on finding whether the volunteers were aware of the concept of ‘inter-individual variability’ by asking them whether they knew that diet could have different effects on different people and about the potential factors involved in these differences.
Data Analysis
Demographic, anthropometric data and questionnaire results were all entered into Excel spreadsheets and analysed through the calculation of summary statistics, frequencies and (or) percentages. Data normality was assessed using the Kolmogorov-Smirnov test. Since most of the variables examined did not fit a normal distribution, results are presented as the median and the 95% CI (lower and upper confidence limits for the median value) and statistical analyses were carried out applying non-parametric tests using the XLSTAT 19.03 software. Where indicated, differences among age and gender subgroups were carried out using the Kruskall–Wallis with Dunn’s post-testing. Analyses of the association between self-reported health concern and associated habits (smoking, alcohol drinking, physical activity) were carried out using a contingency table. The observed frequencies in each subgroup were compared using a Chi-Square test. P-values < 0.05 were considered significant.
Results and Discussion
Anthropometric Characteristics of the Participants
Table 2 summarizes the main anthropometric characteristics of the study participants distributed by age group and gender. In good agreement with previous reports [26, 27] the average BMI, WC, WHR, SBP and DBP values found in our sample population were slightly higher in men than in women and increased with age. A detailed distribution of these values taking into consideration the risk standards for cardio-metabolic disorders development established by the World Health Organization (WHO, 2011) is included in Supplementary Material S2. The results show that a substantial percentage of the participants were in the range of healthy or normal values for each of the markers examined and thus, a 51.5% of the men and a 62.7% of the women had a normal BMI (≥ 18.5–24.99 Kg/m2), 85.4% of men and 86.7% of women had a low risk associated WC (≤ 102 cm for men, ≤ 88 cm for women) and about 69% of men and women also had a good value for WHR (< 0.90 for men, < 0.80 for women). On the other hand, the total % of participants with weight excess (obese + overweight) was 41% of the men and 30% of the women, about 31% of the men and women were in the risk margin of WHR (≥ 0.90 for men, ≥ 0.80 for women) and 10 to 20% of the participants were in the high risk margin for WC. Overall, the % of participants with over-the-limit values for the risk factors examined was slightly inferior to those previously described for the Spanish population [1]. Distribution by age confirmed a BMI rise tendency with age as denoted by an increase in the total percentage of overweight and obese people in the adults as compared with the adolescents, both in men (from 22.2 to 57.1%) and in women (from 23.9 to 44.1%).The percentage of individuals with WC and WHR within the risk margin values was also slightly increased in the adult sample population, more clearly in men. Nevertheless, and in relation to obesity, only 12.6% of the men and 4.0% of the women taking part in the survey exhibited a BMI ≥ 30.0 against 22.8% for men and 20.5% for women reported for the average Spanish population [1]. These differences may be partially explained by the fact that the rate of obesity differs from one Spanish region to another and, in particular, the areas of Madrid and Murcia (where the study was carried out) appear to have slightly lower rates of obesity than other regions [27].
Table 2. Descriptive statistics (median and 95% CI) of the main anthropometric characteristics measured in the sample population: body weight, height, body mass index (BMI), waist circumference (WC), hip circumference, waist-to-hip ratio (WHR), systolic (SBP) and diastolic (DBP) blood pressure in men and women by group age.
|
|
Adolescents
[11–17 y] |
Young adults
[18–40 y] |
Adults
[41–65 y] |
|||
|
|
Median |
(95% CI) |
Median |
(95% CI) |
Median |
(95% CI) |
|
Men |
|
|
|
|
|
|
|
Weight (kg) |
64.3a |
(60.9–72.4) |
74.6b |
(72.2–82.2) |
79.0b |
(76.3–86.0) |
|
Height (cm) |
1.73a |
(1.7–1.8) |
1.74a |
(1.7–1.8) |
1.75a |
(1.70–1.80) |
|
BMI |
20.3a |
(20.2–23.1) |
24.6b |
(23.8–26.8) |
25.6b |
(25.5–28.0) |
|
WC (cm) |
75.5a |
(73.3–80.1) |
83.0b |
(80.3–89.2) |
94.0c |
(90.1–98.3) |
|
Hip (cm) |
94.5a |
(91.9–99.5) |
100b |
(99.4–105.7) |
104.0b |
(101.9–107.1) |
|
WHR |
0.79a |
(0.78–0.82) |
0.82a |
(0.49–0.88) |
0.92b |
(0.87–0.93) |
|
SBP (mm Hg) |
124.5ab |
(121.6–130.2) |
124.0a |
(109.6–133.3) |
135.0b |
(129.5–141.7) |
|
DBP (mm Hg) |
76.5a |
(70.7–78.9) |
77.0a |
(66.5–81.2) |
86.0b |
(82.8–89.5) |
|
Women |
|
|
|
|
|
|
|
Weight (kg) |
56.15a |
(54.2–60.7) |
59.0a |
(58.1–63.2) |
66.5b |
(64.1–71.5) |
|
Height (cm) |
1.60a |
(1.60–1.64) |
1.65a |
(1.63–1.66) |
1.60a |
(1.62–1.67) |
|
BMI |
21.1a |
(20.8–22.8) |
21.0a |
(21.4–23.3) |
24.5b |
(23.9–26.0) |
|
WC (cm) |
71.0a |
(69.3–74.4) |
74.0a |
(72.7–76.9) |
83.0b |
(80.6–87.3) |
|
Hip (cm) |
95.0a |
(91.3–97.0) |
97.5a |
(95.1–100.2) |
102.0b |
(100.2–104.8) |
|
WHR |
0.75a |
(0.74–0.78) |
0.75a |
(0.75–0.78) |
0.81b |
(0.79–0.84) |
|
SBP (mm Hg) |
113.0a |
(105.3–117.7) |
119.0b |
(108.7–122.3) |
124.0b |
(120.3–129.3) |
|
DBP (mm Hg) |
74.0a |
(72.4–78.5) |
78.0a |
(71.1–81.9) |
82.50b |
(79.8–85.2) |
Medians with different letters indicate significant differences between age groups (p<0.05); CI: Confidence Intervals.
Regarding blood pressure, the Spanish hypertensive population has been indicated to reach about 50% in men and 37% in women [3] whereas in our sample, approximately 87% of men and women had normal or optimum SBP values (< 140 mm Hg), 90.6% of women and 76.7% of men had also normal or optimum DBP values (< 89 mmHg) and only about 10–20% of the participants had high SBP and/or high DBP.
Overall, these results indicated that the participants that attended the science event and took part in the survey displayed healthy values for some well-established risk biomarkers (BMI, WC, WHR and blood pressure) suggesting a good metabolic health.
Healthy Consciousness and Lifestyle Habits
The first question (1) of the survey dealt with the self-reported health status. Overall, most participants considered to have a ‘normal’ health (41%) , ‘good’ health (46%) or a ‘very good’ health (9%). Only around 4% indicated to consider having a bad health status. In question 2, participants were asked about their health status. On average, a majority responded affirmatively with 77.3 % of the people marking statement 2 (‘generally concerned’). It has been repeatedly reported that women have in general a greater interest in health, are more worried about their health status and more prompt than men to adopt healthy habits [28]. We explored potential differences between sexes for their self-reported health status (Figures 1a-b) and self-reported health concern (Figure 2a-b) but we did not find significant differences between men and women, at any of the three age groups examined. The self-reported health status was predominantly distributed between normal and good categories for both genders and all age subgroups with only a slightly higher (but not significant) proportion of men than women within the ‘good’ category and a higher proportion of women than men in the ‘normal’ category (Figure 1a-b). Regarding health concern, the adult male participants constituted the largest group generally concerned about their health status whereas, in women, the young adults group was slightly superior to the adolescents and adult groups (Figure 2a-b), but again, this difference was not significant.
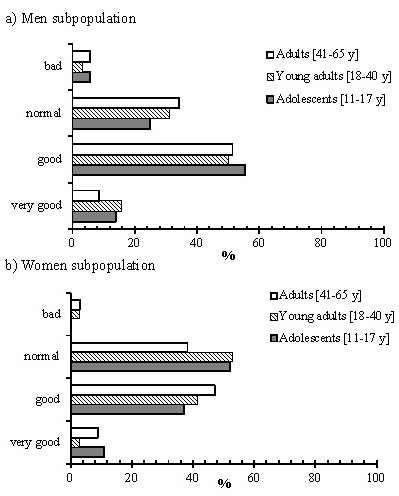
FIGURE 1. Gender and age distribution of the self-reported health status across the sample population.
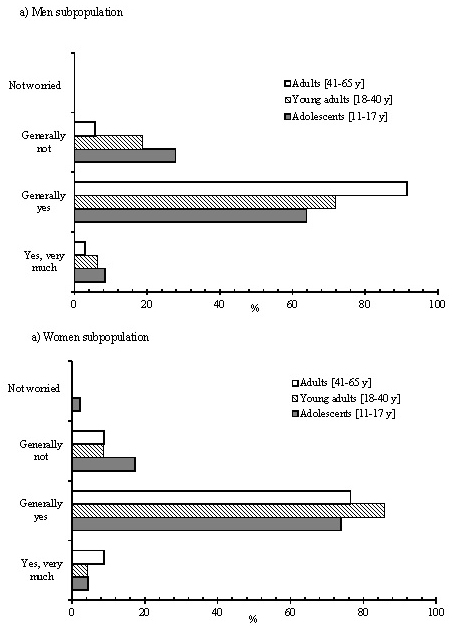
FIGURE 2. Gender and age distribution of the self-reported health concern across the sample population.
In addition to a poor diet, physical inactivity, tobacco use and excessive alcohol consumption are the most relevant modifiable lifestyle habits that are associated with the development of chronic diseases (WHO, 1990). We asked the participants’ about their smoking, alcoholic drinking and sport practicing habits. In general, the consumers subpopulation examined here declared to have good lifestyle habits and was constituted by a majority of non-smokers (80.2%), almost equally divided between occasional/regular consumers of some alcoholic drinks (principally, beer and wine) (50.6%) and not consumers (49.4%). About 75% of the sample population also declared to be active and practiced some physical activity with weekly regularity, mostly aerobic exercise such as walking, cycling, dancing, running, football, gym, swimming, or martial arts. Using a contingency table and a Chi-Square test we investigated a possible relationship between the participant’s self-reported health concern and their consumption of tobacco, alcoholic drinking and physical activity but we did not find any significant relationship (data not shown).
This section of the survey confirmed that, globally, more than 80% of the participants had a positive perception of their health and were concerned about it. These values were higher than the overall 66.6% of positive SRH in the Spanish population [29] reinforcing the healthy orientation of the people who participated in the survey.
General Knowledge About Metabolic Disorders
Questions 3 to 6 of the questionnaire aimed at finding out whether the participants had any general knowledge about some common metabolic disorders, i.e. hypercholesterolemia and hypertension, as well as about type-2 diabetes and metabolic syndrome. The overall results are summarized in Figure 3a-d. Hypertension is a chronic disorder and major risk factor for cardiovascular diseases and has been classically defined as blood pressure readings above 140 and 90 mmHg thresholds for SBP and DBP, respectively [30]. A combination of dietary (high salt consumption), genetic and environmental factors determine a high inter-individual variability in blood pressure values [31]. Hypertension was the most familiar concept for the interviewed volunteers with 77.5% of them affirming to know what hypertension was. Of those, ~95% defined the term as having high blood pressure although very few participants mentioned specific limit values, identified the chronicity of the problem or related it to genetic factors and (or) salt consumption. The rest of affirmative participants (~5%) gave a wrong definition or none. Hypercholesterolemia is also a high prevalent metabolic disorder in the Spanish adult population which is associated with high levels of serum cholesterol and cardiovascular diseases development [2]. Nearly 60% of the participants were also able to recognize and define hypercholesterolemia as high levels of cholesterol in blood although only a few people mentioned limit values or established a link between hypercholesterolemia and bad dietary habits or other factors. In association with high blood pressure and high cholesterol, type-2 diabetes also shows a high prevalence in the Spanish adult population [4]. This complex metabolic disorder is characterized by high glucose levels in blood (hyperglycemia) associated with insulin resistance and pancreatic β-cells alterations [32]. Among the participants, knowledge of type-2 diabetes was slightly inferior to that of the previous disorders since only 47% of the interviewed people responded affirmatively to this question. A miscellaneous of definitions were given: around 37% of the people recognized diabetes as a problem of the pancreas and insulin, about 27% related it with high glucose/sugar levels in blood and nearly 24% defined it as a problem associated with weight and diet and with an excessive consumption of sugar. MetS has been defined as the concurrence of at least three of the following cardio-metabolic risk factors: central obesity, hyperglycemia, hypertension and dyslipidemia [33]. In contrast to the knowledge on some of the previous individual risk factors examined, most of the participants (~80%) have not heard or did not know about MetS, and from the remaining 20% who declared to know this syndrome, very few were able to give a proper or approximate definition with less than 20% describing it as a combination of several factors, i.e. high blood pressure, obesity, high glucose and lipids alteration or as a problem associated with bad dietary habits. A very limited awareness of MetS has been indicated for the general population in other countries such as Greece [34]. This is somehow not surprising since MetS is a very complex and multifactorial disorder. Even university students’ knowledge about MetS and conditions related has been reported to be susceptible to improvement and that raising awareness about MetS remains essential to enhance wellness [35].
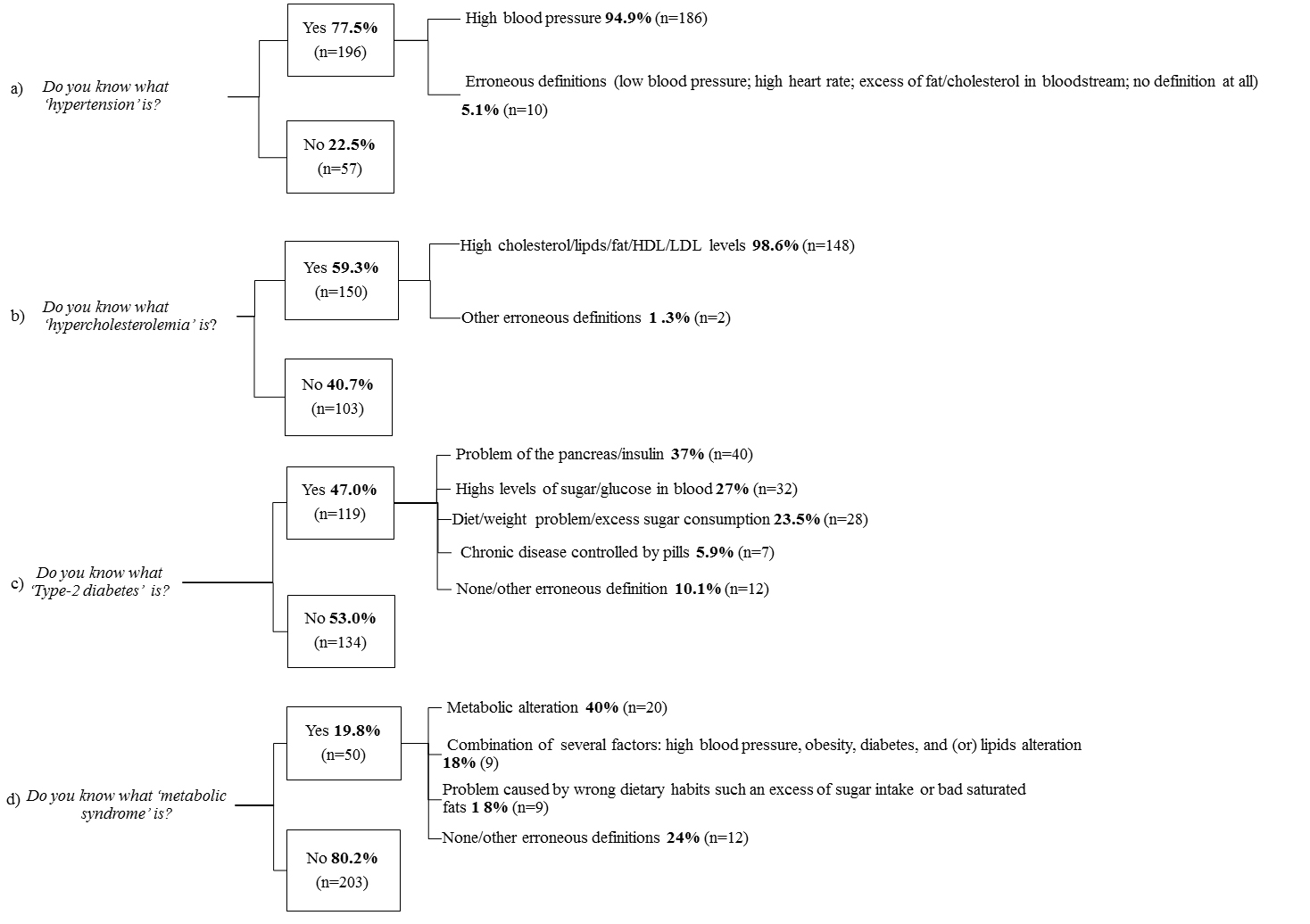
FIGURE 3. Percentage distribution in the sample population of their general knowledge about some common cardio-metabolic risk factors or disorders: a) hypertension, b) hypercholesterolemia, c) type-2 diabetes and d) metabolic syndrome. Some of the definitions given by the participants are also summarized.
On the whole, it appears that the general population has insufficient knowledge about chronic diseases and their associated risk factors. This has important implications for the prevention of these diseases since a better knowledge and understanding of health and disease-related information will influence the health-related behavior and attitude [36].
Health and Diet
A very high proportion of the consumers taking part in this study (93.5%) agreed on that food has an important effect on our health (question 7). The next three questions of the survey referred to the general perception of what a healthy diet was. The distribution of choices selected by the participants is depicted in Figure 4a-c. The most voted responses to question 8 (how the quantity of food we eat affects our health) was number 2 (224 votes, 59.3% of the total votes) followed by number 1 (95 votes, 25.1% of the total votes) (Figure 4a) indicating that a considerable proportion of the participants were aware of the healthiness of eating less quantities of food rather than large quantities. With respect to question 9 (what was generally considered a healthy diet), the three most voted responses ranked in order were 3 (184 votes, 38.2% of the votes), 1 (159 votes, 33% of the votes) and 2 (127 votes, 26.3% of the votes) (Figure 4b) showing that about 57% of the participants were also aware of the importance of eating a diverse diet that included fruits, vegetables, cereals, nuts and olive oil vs. lower intake of meat, fat, salt, sugar and alcohol. Regarding whether the participants thought their habitual diet was healthy (question 10, Figure 4c), the two most voted responses were number 2 (142 votes, 47.8% of the total votes) and number 3 (97 votes, 32.7% of the votes) indicating that they believed to follow the general dietary recommendations. Nevertheless, an important proportion of the participants (~45%) admitted that sometimes they would eat more than they should do. This last statement may be attributed to social and cultural behaviors that critically influence our eating choices and indicate that nutrition knowledge and awareness is necessary but not sufficient to change consumer´s food behaviors [37].
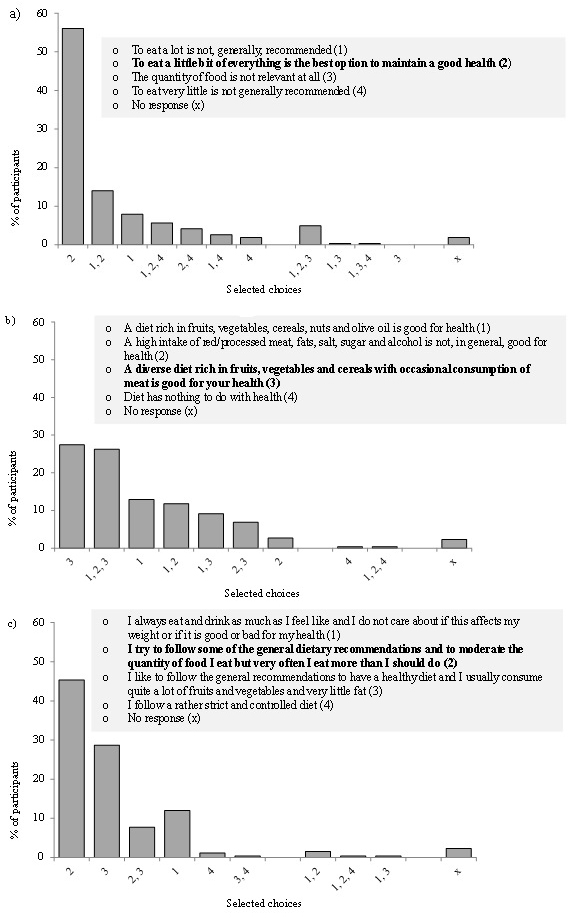
FIGURE 4. Distribution of choices selected by the participants in response to questions 8, 9 and 10 about the relationship between diet & health.
Overall, the participants in this study showed to be generally aware of the importance of diet in health. Previous studies have indicated that women are more health-conscious and more receptive and motivated to food and health issues than men [38]. We, however, did not find any significant differences between men and women’s awareness of the link between diet and health. Gender-related differences are based on a complex network of factors that need to be further investigated to fully understand the role of gender on the perception and adoption of healthy habits [28]
Perception of Functional Foods and Nutraceuticals
It is recognized that to combat the metabolic chronic disorders the use of Functional Foods and Nutraceuticals, both products placed in the interface between pharma and nutrition, may offer opportunities to reduce the risk of developing these diseases [16]. These products may be interesting for those consumers willing to move into healthier habits without making major changes in their food preferences [39]. Some of these products are currently available in the market. Nevertheless, their use is not always clearly stated and (or) regulated nor the general public is aware of or has a good knowledge about them. The results of our survey about the knowledge and consumption of Functional Foods and Nutraceuticals (questions 11 to 20 of the survey) are summarized in Table 3.
Table 3. Total distribution of the responses for questions 11 to 20 of the questionnaire related to the knowledge and consumption of Functional Foods and Nutraceuticals.
|
Summary of Responses to questions 11 to 20 |
Functional Foods |
Nutraceuticals |
||||
|
Do you know what these products are? |
49.6%
(yes) |
48.1%
(no) |
2.3%
(no reply) |
12.9 %
(yes) |
82.2%
(no) |
4.9%
(no reply) |
|
Are you a consumer? |
25.8%
(yes) |
47.3%
(no) |
26.9%
(no reply) |
4.7%
(yes) |
65%
(no) |
30.4%
(no reply) |
|
If your answer was ‘yes’: |
Total votes |
% of total |
Total votes |
% of total |
||
|
10 |
13.9 |
2 |
14.3 |
||
|
5 |
6.9 |
2 |
14.3 |
||
|
12 |
16.7 |
0 |
0 |
||
|
3 |
4.2 |
0 |
0 |
||
|
14 |
19.4 |
2 |
14.3 |
||
|
24 |
33.3 |
5 |
35.7 |
||
|
4 |
5.6 |
3 |
21.4 |
||
|
|
||||||
|
If your answer was ‘no’: |
Total votes |
% of total |
Total votes |
% of total |
||
|
1 |
0.5 |
1 |
0.6 |
||
|
12 |
5.8 |
23 |
13.7 |
||
|
36 |
17.5 |
24 |
14.2 |
||
|
4 |
1.9 |
4 |
2.4 |
||
|
38 |
18.5 |
19 |
11.2 |
||
|
98 |
47.6 |
11 |
6.5 |
||
|
17 |
8.3 |
87 |
51.5 |
||
Nearly half of the volunteers (49.6%) declared to know what Functional Foods were and from these ones, about 90% attempted to give a description of these products. Nevertheless, among the responses, only ~45% were considered to have some degree of agreement with the general definition: Foods that are beneficial for health and (or) foods that have some extra added components with a benefit on health [16]. Of those participants that gave a definition, only 46% also included an example of these products with the three top examples being: ϖ-3 or dairy products with ϖ-3 (23.5% of all the examples), dairy products with plant sterols (22.1%) and dairy products with probiotics (11.8%). They were all mostly referred as to the commercial brand. Regarding the consumption of Functional Foods only 25.8% of the participants declared to consume or to have consumed these products. The predominant reason given was that they liked them and thought they were good for health (as generally stated in the designated Other responses box). In addition, they also took these products: but they were not really sure if they had any effect (5), and because someone recommended to them or saw them on television (3) or were recommended by a doctor (1).
Concerning Nutraceuticals, only 12.9% of the participants affirmed to know them and, from those, about 79% included also a description of these products but very few definitions were considered to have some agreement with the general concept of Nutraceuticals: Food formulations with components that are beneficial for health [17]. Regarding the consumption of Nutraceuticals, only 4.7% of the participants declared to consume or to have consumed them. Some of the main reasons for taking them were also: recommended by a doctor (1), recommended by the pharmacist or in the herbalist shop (2) or they take them but they were not sure if they really have any effect (5).
Among those individuals who stated not to consume Functional Foods, only 18.5 % declared that they would start taking them in the future if they really worked (response 5) and 17.5% would only take them if they were recommended by the doctor (response 3). About 48% of the participants wrote other various reasons such as I don’t eat them because I believe that healthy food and sports are sufficient to keep us healthy, Perhaps I would try them if I needed them and/or if I learnt more about them. From the participants that stated not to consume Nutraceuticals, only 14.2% would only take them if they were recommended by the doctor and 13.7% would not consume these products due to a lack of knowledge and information about these products.
Overall, the sample subpopulation had poor knowledge about Functional Foods or Nutraceuticals, although they appeared to be more familiar with Functional Foods, especially with commercially available brands. Further, the consumption of these products was also very limited among the sample population. It has been suggested that European consumers may be more critical towards novel foods and food-related information than the USA population [20]. Along these lines, it has been hypothesized that, in particular, Spanish consumers interested in health may not consider necessary to eat this type of foods and they are more prone to consume natural foods on a balanced diet [40]. The success and future of the Functional Food category has been shown to depend on the consumer acceptance of the concept of this type of product and that some important factors to be considered for this are: the taste, the belief in the health benefits and the knowledge and awareness of the concept [20]. The results of our preliminary survey also support the notion that overcoming the lack of knowledge and understanding of these products probably by means of specialized recommendations (doctors, pharmaceutics, herbalists) and increasing the evidence of their health benefits will contribute to increase their consumption and future use by the consumers for health maintenance.
Although the prevention of chronic diseases by natural approaches has increased the focus of attention to Nutraceuticals as an alternative to the classic pharmaceutical approach, the concept of Nutraceuticals remains very confusing among the consumers due to insufficient clinical proofs of their benefits and the lack of proper information to the general public [17]. Our results of the survey also support a very limited knowledge and use of these products in the sample population. In general, it appears that despite the growing evidence of the health-promoting effects of many functional ingredients and Nutraceuticals, most of them are still unknown to most consumers. In support of this statement, recently it was shown that consumers in Denmark had little interest and knowledge about resveratrol, an ingredient already present in some Nutraceuticals and that has been widely and intensively investigated for its potential health benefits [41].
Perception of the Differences Between Individuals and Interest in Research on Diet and Health
Prevention of cardiometabolic chronic disorders by healthy foods and (or) by novel foods and products enriched in healthy components, is still lacking conclusive proof and understanding of their benefits in humans. The evidence is still limited and contradictory, partly due to differences between individuals in their metabolism and in their response regarding cardiometabolic health outcomes. Understanding these differences and identifying the factors implied is an important current area of research in diet and health [42]. It is also equally important that consumers are aware and understand these differences. Question 21 of the questionnaire was designed to attain a first impression of whether the participants had any knowledge of the potential differences between individuals in response to diet as well as of some of the factors that may influence this response. The distribution of answers among the sample population is represented in Figure 5. The two most voted responses were number 2 (145 votes, 33.3% of the total votes) and number 3 (145 votes, 33.3% of the votes) showing that a proportion of the participants were aware of the existence of differences between people in the way they were affected by the diet and, importantly, that the genetic factor was involved in these differences. Overall, knowledge of other potential factors was limited and fragmented as shown by the spread of the choices. Nevertheless, it is worth mentioning that approximately 15% and 8% of the votes pointed at life style and microbiota, respectively, as other potential factors involved in the differences between individuals.
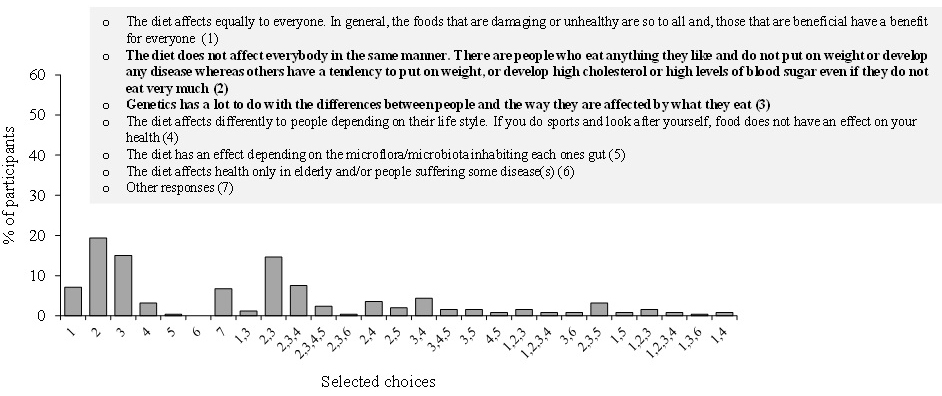
FIGURE 5. Distribution of choices selected by the participants in response to question 21 of the questionnaire about the differences between individuals in response to diet and some of the factors that may influence these differences.
Study Limitations and Main Conclusions
This preliminary study aimed to explore by means of a simple questionnaire, the knowledge and awareness of the participants about several important general issues of the binomial ‘diet and health’. Data were collected from a valid although limited sample of 253 participants who attended the public science event and, in particular, our stand and thus, we acknowledge that the study may be biased towards people with a higher interest in the subject than the general Spanish population.
The survey has confirmed that our sample population had a general good health, was generally concerned about health issues and had reasonably good habits. Although they were generally aware of the relevance of diet to health, their familiarity with chronic metabolic disorders was limited. Further, their knowledge of novel Functional Foods and Nutraceuticals was scarce but they manifested some interest in attaining more information about these products and their efficacy. The concept of inter-individual differences in response to diet was familiar to some but further knowledge of the factors involved was very limited and fragmented.
The results of this survey support the importance and general need to continue providing more and updated information to the population about metabolic health and how to improve it. We should use all possible means (school, university, health centers, consumer’ associations) to expand the information to as many people as possible, both to those that may be more interested and knowledgeable as well as to those who are not so interested on diet and health. It is definitively needed to enhance the understanding about Functional Foods and Nutraceuticals, especially those already freely available in the market. The community of doctors, pharmacists and herbalists also need to be well informed about their advances and applicability so that they can contribute to improve the recommendations and use of these novel food products. Understanding the inter-individual differences in response to diet and, in particular, in response to the beneficial foods and derived products in relation with metabolic disease prevention is an essential area of research. Most participants in the survey agreed on the need to continue these investigations. The results of which need to be translated to the general population to: i) increase their understanding and awareness of the role of diet in health and ii) to contribute further to the prevention of metabolic diseases.
Acknowledgements: BB, MVMA, and MTGC are participants to the European COST Action FA1403 POSITIVe: ‘Interindividual variation in response to consumption of plant food bioactives and determinants involved’. L.L. would like to thank the Spanish “Juan de la Cierva” program for her contract (Ref. FJCI-2014–19907).
References
- Lecube A, et al., (2017) Prevention, diagnosis, and treatment of obesity. 2016 position statement of the Spanish Society for the Study of Obesity. Endocrinología, Diabetes y Nutrición (English ed.) 64: 15–22.
- de la Sierra A, et al. (2015) Prevalence, Treatment, and Control of Hypercholesterolemia in High Cardiovascular Risk Patients: Evidences from a Systematic Literature Review in Spain. Advances in therapy 32: 944–961.
- Menéndez E, et al. (2016) Prevalence, diagnosis, treatment, and control of hypertension in Spain. Results of the Di@ bet. Es study. Revista Española de Cardiología 69: p. 572–578.
- Ena J, et al. (2016) Management of patients with type 2 diabetes and multiple chronic conditions: A Delphi consensus of the Spanish Society of Internal Medicine. European journal of internal medicine 27: 31–36.
- Gavrila D, et al. (2011) Prevalence of metabolic syndrome in Murcia Region, a southern European Mediterranean area with low cardiovascular risk and high obesity. BMC public health 11: 562.
- Jayanti RK, Burns AC (1998) The antecedents of preventive health care behavior: An empirical study. Journal of the Academy of Marketing Science 26: 6.
- Tchicaya A, et al. (2013) Social inequality in awareness of cardiovascular risk factors in patients undergoing coronary angiography. European journal of preventive cardiology 20: 872–879.
- Hsieh CR, Lo TF (2017) Are smokers too optimistic about their health status: Ex ante perception versus ex post observation. China Economic Review 43: 169–183.
- Loprinzi PD (2015)Factors influencing the disconnect between self-perceived health status and actual health profile: implications for improving self-awareness of health status. Preventive medicine 73: 37–39.
- Piotrowicz K, et al. (2015) Self-reported health-related behaviors and dietary habits in patients with metabolic syndrome. Cardiology journal 22: 413–420.
- Cook LA, Burton S, Howlett E (2011) Health risk factors and their effect on consumers’ use of nutrition facts panels. Journal of Consumer Affairs 45: 516–527.
- Parmenter K, Wardle J (1999) Development of a general nutrition knowledge questionnaire for adults. European Journal of Clinical Nutrition 53: 298–308.
- Mingioni M, et al. (2016) Fruit and vegetables liking among European elderly according to food preferences, attitudes towards food and dependency. Food Quality and Preference 50: 27–37.
- Kollajtis-Dolowy A, Zamojcin K (2016) The level of knowledge on nutrition and its relation to health among Polish young men. Roczniki Panstwowego Zakladu Higieny 67: 155–161.
- Alkerwi A, et al, (2015) Association between nutritional awareness and diet quality: evidence from the observation of cardiovascular risk factors in Luxembourg (ORISCAV-LUX) study. Nutrients 7: p. 2823–2838.
- Eussen SR, et al. (2011) Functional foods and dietary supplements: products at the interface between pharma and nutrition. European journal of pharmacology 668: S2-S9.
- Santini A, Tenore GC, Novellino E (2017) Nutraceuticals: A paradigm of proactive medicine. European Journal of Pharmaceutical Sciences 96: 53–61.
- El Sohaimy S (2012) Functional foods and nutraceuticals-modern approach to food science. World Applied Sciences Journal 20: 691–708.
- Urala N, Lähteenmäki L (2004) Attitudes behind consumers’ willingness to use functional foods. Food quality and preference 15: 793–803.
- Verbeke W (2005) Consumer acceptance of functional foods: socio-demographic, cognitive and attitudinal determinants. Food quality and preference 6: 45–57.
- Krystallis A, Maglaras G, Mamalis S (2008) Motivations and cognitive structures of consumers in their purchasing of functional foods. Food Quality and Preference 19: 525–538.
- Axon DR, et al. (2017) Dietary Supplement Use, Knowledge, and Perceptions Among Student Pharmacists. American Journal of Pharmaceutical Education 81: 92.
- Zubeldia Lauzurica L, et al. (2016) Prevalence of Hypertensión and Associated Factors in Population Aged 16 to 90 Years Old in Valencia Region, Spain. Revista espanola de salud publica.
- Ahmed NU, Delgado M, Saxena A (2016) Trends and disparities in the prevalence of physicians’ counseling on diet and nutrition among the US adult population, 2000–2011. Preventive medicine 89: 70–75.
- Santiago S, et al. (2017) Healthy-eating attitudes and the incidence of cardiovascular disease: the SUN cohort. International journal of food sciences and nutrition 68: 595–604.
- Gutiérrez-Fisac J, et al. (2012) Prevalence of general and abdominal obesity in the adult population of Spain, 2008–2010: the ENRICA study. Obesity reviews 13: 388–392.
- Aranceta-Bartrina J, et al. (2016) Prevalence of general obesity and abdominal obesity in the spanish adult population (aged 25–64 years) 2014–2015: The ENPE study. Revista Española de Cardiología (English Edition) 69: 579–587.
- Varì R, et al. (2016) Gender-related differences in lifestyle may affect health status. Annali dell’Istituto Superiore di Sanità 52: 158–166.
- Girón, P (2010) Determinants of self-rated health in Spain: differences by age groups for adults. The European Journal of Public Health 22: 36–40.
- Currie G and Delles C (2016) Use of biomarkers in the evaluation and treatment of hypertensive patients. Current hypertension reports 18: 54.
- Iatrino R, Manunta P, Zagato L (2016) Salt sensitivity: challenging and controversial phenotype of primary hypertension. Current hypertension reports, 18: 70.
- Zaccardi F, et al. (2015) Pathophysiology of type 1 and type 2 diabetes mellitus: a 90-year perspective. Postgraduate medical journal, 2015: p. postgradmedj-2015–133281.
- Grundy S (2005) Metabolic syndrome: therapeutic considerations, in Atherosclerosis: Diet and Drugs. Springer. 107–133.
- Athyros V, et al. (2005) Awareness, treatment and control of the metabolic syndrome and its components: a multicentre Greek study. Hellenic J Cardiol 46: 380–386.
- Yahia N, et al. (2014) Assessment of college students’ awareness and knowledge about conditions relevant to metabolic syndrome. Diabetology & metabolic syndrome 6: 111.
- Webster R, Heeley E (2010) Perceptions of risk: understanding cardiovascular disease. Risk Management and Healthcare Policy 3: 49.
- Worsley A (2002) Nutrition knowledge and food consumption: can nutrition knowledge change food behaviour? Asia Pacific journal of clinical nutrition 11.
- Andrade L, Zazpe I, et al. (2017) Ten-Year Changes in Healthy Eating Attitudes in the SUN Cohort. J Am Coll Nutr 36: 319–329. Williamson AR, Hunt AE, Pope JF, Tolman NM (2000) Recommendations of dietitians for overcoming barriers to dietary adherence in individuals with diabetes. Diabetes Educ 26: 272–279.
- Küster-Boluda I, Vidal-Capilla I (2017) Consumer attitudes in the election of functional foods. Spanish Journal of Marketing-ESIC 21: 65–79.
- Aschemann-Witzel J, Grunert KG (2015) Resveratrol and health from a consumer perspective: perception, attitude, and adoption of a new functional ingredient. Annals of the New York Academy of Sciences 1348: 171–179.
- Manach C, et al (2017) Addressing the inter-individual variation in response to consumption of plant food bioactives: Towards a better understanding of their role in healthy aging and cardiometabolic risk reduction. Molecular nutrition & food research 61.
Supplementary Material S1.- Self-administered questionnaire.
Diet & Health: What’s Your Opinion?
|
Age: Sex: Measurements taken on the day of the questionnaire Weight (Kg): Height (m): BMI:
Waist circumference (cm): Hip circumference (cm): Waist-to-hip ratio:
Sistolic blood pressure (mm Hg): Diastolic blood pressure (mm Hg):
Do you… Smoke? YES / NO (indicate cigarettes consumption, daily or weekly) Drink alcohol? YES / NO (indicate consumption, daily or weekly, quantity and type of drink) Practice sport? YES / NO (indicate what activities/sports you do/practice and frequency)
Please, mark the categories that best describe your situation 1. HOW DO YOU CONSIDER YOUR HEALTH STATUS? Very good, even better than the average status for people of my age (1) Good (2) Normal (3) Bad (4) Very bad, worse than the average status for people of my age* (5) * Please, indicate if, at present, you suffer from any chronic/acute disease:
2. ARE YOU CONCERNED ABOUT YOUR HEALTH STATUS? Yes, I am very much concerned. I dedicate quite some time to the health issue and I often search for information about forefront related topics (1) I am generally concerned about my health and I try to follow a healthy style of life (2) Generally, I do not worry about my health (3) I am not in the least concerned about my health. I simply do not worry about it at all (4) Other responses (Please, indicate them in the box below)
3. Do you know what ‘hypercholesterolemia’ is? NO / YES (Please, use your own words definition)
4. Do you know what ‘hypertension’ is? NO / YES (Please, use your own words definition)
5. Do you know what ‘Type-2 diabetes’ is? NO / YES (Please, use your own words definition) 6. Do you know what ‘metabolic syndrome’ is? NO / YES (Please, use your own words definition)
7. How much do you agree with the next statement? ‘FOOD HAS AN IMPORTANT EFFECT ON MY HEALTH’ I totally agree (1) I agree (2) I don´t agree or disagree (3) I disagree (4) I totally disagree (5)
8. DO YOU KNOW, IN GENERAL, HOW THE QUANTITY OF FOOD AFFECTS OUR HEALTH? (please, mark the statement(s) you agree with) To eat a lot is not, generally, recommended (1) To eat a little bit of everything is the best option to maintain a good health (2) The quantity of food is not relevant at all (3) To eat very little is not generally recommended (4)
9. DO YOU KNOW WHAT IS CONSIDERED, IN GENERAL, A ‘HEALTHY DIET’? (please, mark the statement(s) you agree with) A diet rich in fruits, vegetables, cereals, nuts and olive oil is good for health (1) A high intake of red/processed meat, fats, salt, sugar and alcohol is not, in general, good for health (2) A diverse diet rich in fruits, vegetables and cereals with occasional consumption of meat is good for your health (3) Diet has nothing to do with health (4) Other responses (Please, indicate them in the box below)
10. DO YOU BELIEVE YOUR HABITUAL DIET IS ‘HEALTHY’? (please, mark the statement(s) that best describe your situation) I always eat and drink as much as I feel like and I do not care about if this affects my weight or if it is good or bad for my health (1) I try to follow some of the general dietary recommendations and to moderate the quantity of food I eat but very often I eat more than I should do (2) I like to follow the general recommendations to have a healthy diet and I usually consume quite a lot of fruits and vegetables and very little fat (3) I follow a rather strict and controlled diet (4) Other responses (Please, indicate them in the box below)
11. DO YOU KNOW WHAT FUNCTIONAL FOODS ARE? YES / NO
12. If yes, HOW WOULD YOU DESCRIBE THEM? Can you quote a few examples? Please, indicate them in the box below
13. ARE YOU A CONSUMER OF SOME OF THESE PRODUCTS? YES / NO
14. If your answer was ‘yes’: You take them because your doctor recommended to you (1) You take them because it was recommended to you by the pharmacist or in the herbalist’s shop (2) You take them because someone recommended to you or you saw it on TV (3) You take them because you like it although you think they are not very useful (4) You take them although you are not sure if they really have an effect (5) Other responses (Please, indicate your own opinion about these foods in the box below)
15. If your answer was ‘no’: I have no intention of consuming these functional foods since I do not believe they work (1) I will not consume these functional foods because I do not know what they are (2) I would only take them it they were recommended to me by the doctor (3) I would start eating them only if they were tasty (4) Maybe, I will start taking them in the future if they really work (5) Other responses (Please, indicate your own opinion about these foods in the box below)
16. DO YOU KNOW WHAT NUTRACEUTICALS ARE? YES/NO
17. If yes, HOW WOULD YOU DESCRIBE THEM? Can you quote a few examples? Please, indicate them in the box below
18. ARE YOU A CONSUMER OF SOME OF THESE PRODUCTS? YES / NO
19. If your answer was ‘yes’: You take them because your doctor recommended to you (1) You take them because it was recommended to you by the pharmacist or in the herbalist’s shop (2) You take them because someone recommended to you or you saw it on TV (3) You take them because you like it although you think they are not very useful (4) You take them although you are not sure if they really have an effect (5) Other responses (Please, indicate your own opinion about these products in the box below)
20. If your answer was ‘no’: I have no intention of consuming these nutraceuticals since I do not believe they work (1) I will not consume these nutraceuticals because I do not know what they are (2) I would only take them it they were recommended to me by the doctor (3) I would start eating them only if they were tasty (4) Maybe, I will start taking them in the future if they really work (5) Other responses (Please, indicate your own opinion about these foods in the box below)
21. DO YOU THINK THAT THE DIET HAS THE SAME EFFECTS ON EVERYBODY? (please, mark the statement(s) that best describe your opinion) The diet affects equally to everyone. In general, the foods that are damaging or unhealthy are so to all and, those that are beneficial have a benefit for everyone (1) The diet does not affect everybody in the same manner. There are people who eat anything they like and do not put on weight or develop any disease whereas others have a tendency to put on weight, or develop high cholesterol or high levels of blood sugar even if they do not eat very much (2) Genetics has a lot to do with the differences between people and the way they are affected by what they eat (3) The diet affects differently to people depending on their life style. If you do sports and look after yourself, food does not have an effect on your health (4) The diet has an effect depending on the microflora/microbiota inhabiting each ones gut (5) The diet affects health only in elderly and/or people suffering some disease(s)(6) Other responses (Please, indicate your own opinion about these foods in the box below)
|
Supplementary Material S2. Distribution of the anthropometric characteristics of the sample population taking into consideration the values established by the World Health Organization (WHO) to differentiate between low risk and high risk for cardio-metabolic disorders development.
|
|
|
Total sample population n (%) |
Adolescents [11–17 y] n (%) |
Young adults [18–40 y] n (%) |
Adults [41–65 y] n (%) |
|
Men |
|||||
|
BMI (Kg/m2) |
< 18.5 (low weight) |
8 (7.8) |
8 (22.2) |
0 (0.0) |
0 (0.0) |
|
≥ 18.5–24.99 (normal weight) |
53 (51.5) |
20 (55.5) |
18 (56.3) |
15 (42.9) |
|
|
≥ 25.0–29.99 (overweight) |
29 (28.2) |
7 (19.4) |
9 (28.1) |
13 (37.1) |
|
|
≥ 30.0 (obesity) |
13 (12.6) |
1 (2.8) |
5 (15.7) |
7 (20.0) |
|
|
WC (cm) |
≤ 102 cm (low risk) |
88 (85.4) |
33 (91.7) |
27 (84.3) |
28 (80.0) |
|
> 102 cm (substantially increased risk) |
15 (14.6) |
3 (8.3) |
5 (15.7) |
7 (20.0) |
|
|
WHR |
< 0.90 (good) |
71 (68.9) |
25 (69.4) |
23 (71.9) |
23 (65.7) |
|
≥ 0.90 (substantially increased risk) |
32 (31.1) |
11 (30.6) |
9 (28.2) |
12 (34.3) |
|
|
SBP (mm Hg) |
≤ 120 mm Hg (optimum) |
37 (35.9) |
20 (55.5) |
11 (34.4) |
6 (17.1) |
|
121–139 mm Hg (normal) |
53 (51.5) |
14 (38.9) |
13 (40.7) |
26 (74.3) |
|
|
≥140 mm Hg (high) |
13 (12.6) |
2 (5.6) |
8 (25.0) |
3 (8.6) |
|
|
DBP (mm Hg) |
≤ 80 mm Hg (optimum) |
42 (40.8) |
26 (72.2) |
12 (37.5) |
4 (11.4) |
|
81–89 mm Hg (normal) |
37 (35.9) |
6 (16.7) |
13 (40.7) |
18 (51.4) |
|
|
≥ 90 mm Hg (high) |
24 (23.3) |
4 (11.1) |
7 (21.9) |
13 (37.1) |
|
|
Women |
|||||
|
BMI (Kg/m2) |
< 18.5 (low weight) |
13 (8.7) |
6 (13.0) |
7 (10.0) |
0 (0.0) |
|
≥ 18.5–24.99 (normal weight) |
94 (62.7) |
29 (63.0) |
46 (65.7) |
19 (55.9) |
|
|
≥ 25.0–29.99 (overweight) |
37 (24.7) |
10 (21.7) |
14 (20) |
13 (38.2) |
|
|
≥ 30.0 (obesity) |
6 (4.0) |
1 (2.2) |
3 (4.3) |
2 (5.9) |
|
|
WC (cm) |
≤ 88 cm (low risk) |
130 (86.7) |
37 (80.4) |
64 (91.4) |
29 (85.3) |
|
> 88 cm ( substantially increased risk) |
20 (13.3) |
9 (19.6) |
6 (8.6) |
5 (14.7) |
|
|
WHR |
< 0.80 (good) |
103 (68.7) |
31 (67.4) |
50 (71.4) |
22 (64.7) |
|
≥ 0.80 (substantially increased risk ) |
47 (31.3) |
15 (32.6) |
20 (28.5) |
12 (35.3) |
|
|
SBP (mm Hg) |
≤ 120 mm Hg (optimum) |
70 (46.7) |
24 (52.2) |
33 (47.1) |
13 (38.2) |
|
121–139 mm Hg (normal) |
60 (40.0) |
18 (39.1) |
27 (38.6) |
15 (44.1) |
|
|
≥ 140 mm Hg (high) |
20 (13.3) |
4 (8.7) |
10 (14.3) |
6 (17.6) |
|
|
DBP (mm Hg) |
≤ 80 mm Hg (optimum) |
89 (59.3) |
32 (69.6) |
46 (65.7) |
11 (32.4) |
|
81–89 mm Hg (normal) |
47 (31.3) |
11 (23.9) |
19 (27.1) |
17 (50.0) |
|
|
≥ 90 mm Hg (high) |
14 (9.3) |
3 (6.5) |
5 (7.1) |
6 (17.6) |
|