There is still much controversy surrounding the mechanisms that produce orbital blowout fractures. Since the first report of blowout fracture, theories have evolved and experiments been conducted to elucidate and demonstrate three mechanisms which are the globe-to-wall contact, hydraulic, and buckling.
Erling et al [1] resurrected older mechanism on the etiology of inferomedial orbital fractures first espoused by Pfeiffer [2] in 1943. They proposed that the responsible mechanism of inferomedial orbital fracture is a direct globe-to-wall contact; that is, posterior movement of the globe, in response to an external force, results in a fracture upon direct contact with an orbital wall. They investigated CT scans of blowout fractures of the pure medial and inferomedial wall, demonstrated that the size of the orbital displacement exactly fitted the shape of the globe in many cases. We also examined the charts of estimated 45 cases of this mechanism for the clinical information. According to Erling’s description [1], CT scans were reviewed by overlaying a tracing of the globe displaced directly down the longitudinal orbital axis to evaluate the likelihood of posterior globe displacement as a mechanism of fracture. The size of the orbital wall displacement exactly fit the globe in 46.7 % (20/45) patients [3] (Figure 1). All fractures were occurred in the inferomedial area of the orbital wall. In our study, serious complications like corneal laceration, globe rapture, 3rd cranial nerve paralysis, and ophthalmic nerve neuropathy plus 3rd, 4th, 6th cranial nerve paralysis (Orbital Apex Syndrome) were seen more frequently than other reports. These serious complications seem great impact had acted the globes. It is necessary to take enough care for delayed neuropathy, when CT scan of patient shows orbital fracture due to “globe-to-wall contact mechanism”, even if he dose not complain any symptom immediate after injury.
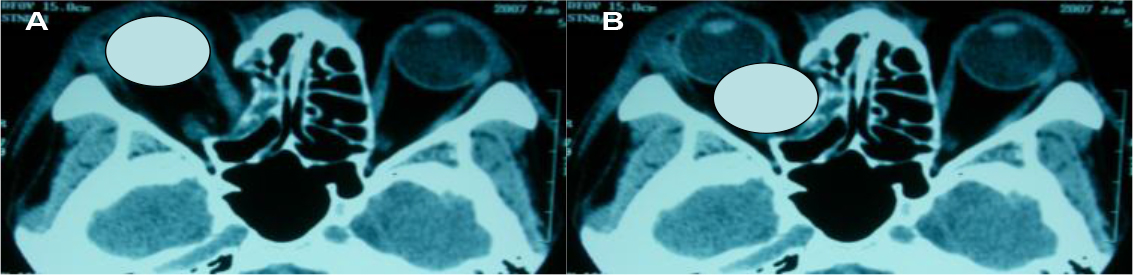
Figure 1. A-53-year man fell down and hit the right eye region to the floor. The CT finding showed the displacement of the right inferomedial wall. The size of the orbital wall displacement exactly fit the globe (A, B).
There is no doubt that almost blowout fractures of the orbit could be due to a single mechanism alone or a combination of 2 or more mechanisms clinically [4]. We conclude that “globe-to-wall contact mechanism” advocated by Pfeiffer acts in some respect to making fracture formation in some orbital blowout fractures in the inferomedial area of the orbital wall.
Key words
Blowout Fracture; Orbital Fracture; Globe-to-Wall Contact Mechanism.
References
- Erling BF, Iliff N, Robertson B, et al. (1999) Footprints of the globe: a practical look at the mechanism of orbital blowout fractures, with a revisit to the work of Raymond Pfeiffer. Plast Reconstr Surg 103: 1313–1316.
- Pfeiffer RL (1943) Traumatic enophthalmos. Arch Ophthalmol 30: 718–726.
- Sugamata A, Yoshizawa N (2010) Clinical analysis of orbital blowout fractures caused by a globe-to-wall contact mechanism. J Plast Surg Hand Surg 44: 278–281.
- Sugamata A (2014) Etiology of orbital blowout fractures. J Tokyo Med Univ 72: 19–24.