Abstract
Background: SARS-CoV-2 is the pathogenic agent of COVID-19, which has affected more than 200 countries; infected over 4 million people and declared a global pandemic. At the time of writing, no approved definitive therapeutic treatment for COVID-19 is available. Many studies are still on-going. Lopinavir-ritonavir (LPV/r), or its combination has been advocated as a potential treatment. This study reviews the evidence of LPV/r usage in the treatment of SARS-CoV-2 infection.
Methods: A systematic review protocol was written based on the PRISMA Statement Article for review selected from electronic databases (PubMed, Embase and Medline). Inclusion criteria were: full English articles published between 2019 and 2020, accessible and peer-reviewed. The search keywords were: Lopinavir, COVID, and SARS-CoV-2. Studies fulfilling the inclusion criteria were included, regardless of study designs. Data were extracted from published reports.
Findings: As of 9 May 2020, 243 manuscripts were identified. Thirteen studies were included with a total of 494 patients. These consisted of clinical trials (n=2), case reports (n=5), case series (n=3), and retrospective cohort studies (n=3). In the thirteen studies, the use of LPV/r shortened the PCR negative-conversion time for SARS-CoV-2, the earliest as being 5 days (Range: 5 to 28 days), and clinical improvement was expected as early as 2 days (Range: 2 to 28 days).
Interpretation: Our review shows that the use of LPV/rmay be an effective treatment for non-severe COVID-19 patients, while only limited benefits were observed in severe COVID-19 patients.
Introduction
Coronavirus disease in 2019(COVID-19) is caused by SARS-CoV-2 infection, first reported from Wuhan, China in early December 2019 [1]. It spreads quickly with a reproductive number R0 between 2.2 [2] and 5.7 [3]. It has been declared a pandemic with over 200 countries affected [4]. More than 4 million patients have been infected, resulting in over 250,000 deaths (6.93% case-fatality rate) as of May 10, 2020 [5]. However, there is no definite effective treatment and vaccine against COVID-19. SARS-CoV-2 is a positive-sense single-stranded RNA virus with a diameter of 60-140nm [6]. It is a beta-coronavirus which includes MERS-CoV and SARS-CoV. It is believed to be zoonotic in origin, with close genetic linkage to bat coronavirus. The incubation period is 1-14 days, transmitted through droplets and close contacts [7]. Lopinavir and ritonavir (LPV/r) are protease inhibitors for treating HIV infection. Lopinavir is used in fix-dosage combination with ritonavir to increase bioavailability. LPV/r has been used in the treatment of SARS-CoV and MERS-CoV infection, with effective outcomes [8]. Preliminary research supported the use of LPV/r in COVID-19. It has been recommended by the Chinese Centre for Disease Control and Prevention(CDC) since their third amendment of guidelines [7]. Previously, an inconclusive rapid review was published [9]. Since then more studies have been performed on efficacy of LPV/r for COVID-19 from other Asian [10-14] and European countries [15]. This prompts a more comprehensive review. In this review, we included a summary review of thirteen studies on the usage of LPV/r for treatment of COVID-19, exploring its clinical efficacy, adverse events, and usage in special populations. The strengths and limitations of these studies will be discussed.
Methods
Search Strategy and Selection Criteria
The target reports of this review were peer-reviewed English articles that are accessible on the three electronic databases (PubMed, Embase, Medline). We limited the search period between 2019 and 2020. All patients included in the studies had COVID-19 infection confirmed by PCR testing. A systematic review protocol was written on the basis of PRISMA 2009 guidelines. The search keywords were lopinavir, COVID-19 and SARS-CoV-2. All existing literature with therapeutic data on the use of LPV/r for COVID-19 were included. Database outputs were combined to address the key issues:
1. The documentation of LPV/r for COVID-19 patients in clinical practice, regardless of patient characteristics, countries of residence, clinical settings and outcome measures.
2. Clinical outcomes of the treatment (recovery, mortality) and side effects, especially for special populations.
Study Selection and Validity Assessment
All papers fitting the inclusion criteria were selected and analysed. The inclusion criteria were:
1. Peer-reviewed English article with therapeutic data.
2. Accessible on the databases. (PubMed, Embase and Medline)
3. Published between 2019 and May 9 2020.
The titles, abstracts and full articles were independently screened by the authors. Following the PRISMA guidelines in PRISMA flow diagram, the study profile is shown in Figure 1. Duplicate articles were removed, and reasons for exclusions are documented in the table in Appendix. Quality assessments were assessed by CASP appraisal on each study (if appropriate). Bias or quality issues were minimized by cross-checking of quality assessments by the authors.
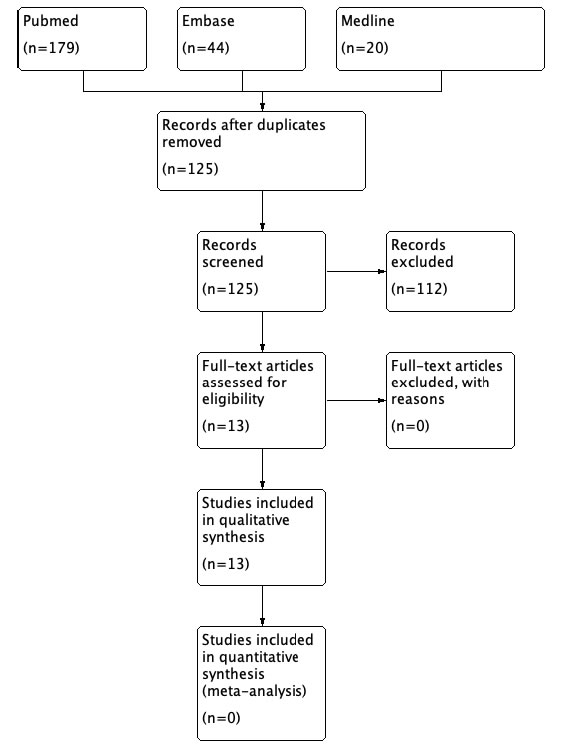
Figure 1. Study profile (PRISMA Flow Diagram).
Data Extraction and Bias Assessment
Data extraction was performed by Zhipeng Yan and Ching-Lung Lai with specific focus on: study design, population demographics, therapeutic outcomes, adverse events and other key findings (if appropriate). The principal source of potential bias was the lack of standardization of outcome measures: viral loads were measured after different days of treatment with LPV/r, usually without continuous monitoring. This review used a time-interval approach, with 5-days units, to assess the time for patients to become negative for PCR test for SARS-CoV-2. Patient recovery was classified into six different groups: 1-5 days, 6-10 days, 11-15 days, 16-20 days, 21-25 days and 26-30 days. Assessment was based on the reported data; without authors for extra or missing information.
Data Analysis
The following were analysed to assess the efficacy of LPV/r in COVID-19 patients: the time to obtain a negative-conversion of PCR test for SARS-CoV-2 and the number of adverse events affecting different systems. All analyses were conducted using Microsoft Excel 2013.
Results
As of 9 May, 2020, 243 articles were identified initially. Using the PRISMA guidelines, the reasons for inclusion and exclusion are presented in a PRISMA flow diagram (Figure 1).
Thirteen studies were finally included (Table 1) :randomised clinical trial (n=2), case reports (n=5), retrospective cohort study (n=3), and case series (n=3). Ten out of the thirteen (76.9%) studies were conducted in China including Hong Kong, and one each from Italy, South Korea and Spain.A total of 494 patients were reported in the studies. The mean age was 52.8 years (excluding the seventh study in Table 1 because data on age were not complete). The outcome measures included time to clinical improvements, days to achieve negative-conversion in PCR detection for SARS-CoV-2 and mortality (Tables 1 and 2).
|
Table 1: Summary of the thirteen selected studies. |
||||||||||
|
|
Name of the study |
Cityandcountry |
Sample size |
Age(mean) |
Gender |
Type of study |
Therapeutic treatment |
Type/Number of patients & % |
Outcomes(recovery/mortality) |
Quality assessment(applicable/inapplicable) |
|
1 |
Cao, B., Wang, Y., Wen, D., et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19. N Engl J Med 2020. May 7. DOI:10.1056/NEJMoa2001282 |
Wuhan,China |
199 |
58 Y |
120 M |
Randomized |
LPV/r |
LPV/r:
Standard Care: |
-No benefit was observed with LPV/r treatment beyond standard care in severe COVID-19 patients. -19 patients on intervention arm died. -3 premature deaths in LPV/r group within 24 hours after randomization |
-A focused issue addressed. -Randomization performed with intention-to-treat analysis. -Population were properly accounted their inclusion -Not blinded. -Baseline demographics was similar in both groups. -Primary outcome clearly specified. -Showed little benefits without statistical significance. -Total 5 patients dropped out: 3 premature death, 2 failedprescriptions of LPV/r by physician. |
|
2 |
Hung IFN LK, Tso EYK, et al. Triple combination of interferon beta-1b, lopinavir–ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: an open-label, randomised, phase 2 trial. Lancet. 2020.May 8. |
Hong Kong, |
127 |
52 Y |
68 M |
Randomised controlled trial |
LPV/r + |
LPV/r + IFN-ß + ribavirin:
LPV/r control group:
|
-Triple therapy group had a significantly shorter median time for negative-conversion PCR test for SARS-CoV-2: -Triple therapy group achieved a significantly shorter median time to National Early Warning Score 2 (NEWS2) of 0: -Triple therapy achieved a significantly shorter median time to Sequential Organ Failure Assessment (SOFA) score to reach zero: -Shorter median duration of stay in triple therapy group: -No patient died. |
-A focused issue addressed. -Randomization performed. -Population were properly accounted their inclusion. -Not blinded. -Baseline demographics was similar in both groups. -Primary outcome clearly specified. -Secondary outcome clearly specified. -1 patient in control group dropped out due to biochemical hepatitis.
|
|
3 |
Righi, G., & Del Popolo, G. COVID-19 tsunami: the first case of a spinal cord injury patient in Italy. Spinal Cord Ser Cases 2020, 6: 22. |
Firenze, |
1 |
56 Y |
1 M |
Case report |
LPV/r, and HCQ† |
LPV/r and HCQ: |
-Fever subsided 2 days after treated with LPV/r and HCQ. -Low-dose oxygen therapy was not required 3 days after treated with LPV/r and HCQ. |
-Use of combination treatment that masked the real therapeutic outcome of LPV/r. -In contrast to the spinal cord injury-induced immune depression syndrome, the patient was discharged with complete healing within 2 weeks. -Reported that absence of cough as the presenting symptoms in spinal cord injury. -Only one case. -Side effects of medication not reported. |
|
4 |
Lim, J., Jeon, S., Shin, H. Y., et al. Case of the Index Patient Who Caused Tertiary Transmission of COVID-19 Infection in Korea: the Application of Lopinavir/Ritonavir for the Treatment of COVID-19 Infected Pneumonia Monitored by Quantitative RT-PCR. J Korean Med Sci 2020, 35: e79. |
Goyang, |
1 |
54 Y |
1 M |
Case report |
LPV/r |
LPV/r: |
-Fever subsided 5 days after treatment with LPV/r. -Undetectable viral load since the second day after taking LPV/r. |
-Difficult to determine whether recovery was due to natural cause or use of LPV/r, due to the late administration of drugs. -Only one case. |
|
5 |
Fernandez-Ruiz, M., Andres, A., Loinaz, C., et al. COVID-19 in solid organ transplant recipients: a single-center case series from Spain. Am J Transplant 2020. Apr 16. |
Madrid, |
18 |
71 Y |
14 M |
Single centre retrospective |
LPV/r HCQ IFN-ß IVIg‡ Tocilizumab No antivirals |
LPV/r: LPV/r + HCQ: LPV/r + HCQ + IFN-ß:
HCQ: HCQ + IVIg: HCQ + IFN-ß:
no anti-viral: |
-A total of 5 deaths: 4 receiving LPV/r died, and 1 receiving standard care without anti-viral agent died. -For patients on HCQ, 2 showed clinical improvements, 1 showed mild ARDS, 1 showed persistent respiratory failure and 1 died. -For patients on LPV/r together with HCQ, 2 showed clinical improvement and discharged. The other 3 showed persistent respiratory failure, mild ARDS and death respectively. -The patient on HCQ and IVIg was discharged. -The patients on LPV/r, HCQ and IFN-ß were discharged home. -Patients received no antivirals resulted in 1 death and 1 low-grade fever till the end of study.
|
-Small sample size. -No numerical data provided to tell the efficacy of drugs by measurement of viral load change during the study. -Single centre. -Only 2 patients performed cytokine study. -Side effect of drugs not reported. |
|
6 |
Tang, B., Li, S., Xiong, Y., et al. Coronavirus Disease 2019 (COVID-19) Pneumonia in a Hemodialysis Patient. Kidney Med 2020. Mar 12. DOI::10.1016/j.xkme.2020.03.001 |
Zhongshan, |
1 |
50 Y |
1 M |
Case report |
LPV/r and moxifloxacin |
LPV/r: |
-Nucleic acid test of SARS-CoV-2 turned negative in throat swab after 8 days of treatment. -No observable side effects of LPV/r. |
-Only one case. -Use of moxifloxacin might masked the real therapeutic effect of LPV/r.
|
|
7 |
Ye, X. T., Luo, Y.L., |
Rui’an, |
47 |
9 under 30 Y 38 over 30 Y
|
22 M |
Single centre retrospective cohort study |
LPV/r Adjuvant drugs§ |
LPV/r: Adjuvant drugs: |
-Fever subsided earlier in test group. -Shorter SARS-nCoV-2 RNA negative conversion time in test group. -No observed liver toxicity. |
-Single centre study. -Unbalanced treatment arm and control arm.
|
|
8 |
Wang, Z., Chen, X., |
Shanghai, |
4 |
44.3 Y |
3 M |
Single centre |
LPV/r Arbidol SFJDC¶
|
All received LPV/r, arbidol or SFJDC; or a combination of them. Detailed distribution was not provided. |
-2 patients discharged with confirmed negative PCR on 2 consecutive throat swab 2019-nCoV test. -1 patient was negative on the first virus testing of 2019-nCoV. -All patients showed chest radiography improvement after 5-15 days of taking -Side effects of medication were not observed.
|
-Failed to mention exact regime for each patient. -Small sample size to assess the effect of combined Chinese and western medicine treatment for COVID-19.
|
|
9 |
Liu, F., Xu, A., Zhang, Y., et al. Patients of COVID-19 may benefit from sustained lopinavir-combined regimen and the increase of eosinophil may predict the outcome of COVID-19 progression. Int J Infect Dis 2020. Mar 12.DOI:10.1016/j.ijid.2020.03.013 |
Hangzhou |
10 |
42 Y |
4 M |
Single centre retrospective |
LPV/r IFN-ß:
|
LPV/r + IFN-ß: LPV/r: |
-The patient on LPV/r alone was discharged after 3 days of treatment. -3 patients on LPV/r + IFN-ß developed serious complications, persistent SARS-CoV-2 RNA PCR test positive and were transferred to more specialised unit, all presented with low eosinophil counts. -5 patients on “LPV/r + IFN-ß” developed severe O2 desaturation <93%. -No reported acute myocardial injury nor acute kidney injury. |
-Small sample size in a single centre. -Failed to provide the treatment details and subsequent clinical progress of the 3 transferred patients. |
|
10 |
Han, W., Quan, B., Guo, Y., et al.The course of clinical diagnosis and treatment of a case infected with coronavirus disease 2019. J Med Virol 2020, 92: 461-463. |
Wuwei, |
1 |
47 Y |
1 M |
Case report |
LPV/r Steroid IFN-α2b|| Ambroxol Moxifloxacin |
LPV/r: |
-PCR tests for -Discharged on day 10 with no reported complications during treatment period. |
Failed to address whether the clinical improvement was due to LPV/r or other drugs. |
|
11 |
Zhu, Z., Lu, Z., Xu, T., |
Changzhou |
50 |
36.0 Y |
26 M |
Retrospective cohort study |
LPV/r Arbidol |
LPV/r: Arbidol: |
-None developed severe pneumonia or ARDS. -On day 7 after treatment, higher percentage of patients with undetectable viral load in Arbidol group (50%) vs. LPV/r group (23.5%). -On day 14 after treatment, all patients were with undetectable viral load in Arbidol group (100%) vs. LPV/r group (55.9%). -Patients with arbidol had a shorter duration of RNA positive period. (p<0.01) |
Unbalanced treatment arm and control arm.
|
|
12 |
Deng, L., Li, C., Zeng, |
Zhuhai |
33 |
44.6 Y |
17 M |
Retrospective cohort study |
LPV/r LPV/r + arbidol |
LPV/r: LPV/r + arbidol: |
-On day 7, more patients were tested PCR negative for SARS-CoV-2 in respiratory sample in combination group [12/16 (75%) patients] than monotherapy group [6/17 (35%) patients]. -On day 14, more patients were tested PCR negative for SARS-CoV-2 in respiratory sample in combination group [15/16 (94%) patients] than monotherapy group [9/17 (53%) patients] |
-Small sample size. -Non-randomized study. -Selection and unmeasured confounding bias. |
|
13 |
Wang L, Xu X, Ruan J, |
Fujian |
2 |
54.5 Y |
1 M |
Case report |
LPV/r + arbidol + Lianhuaqingwen + |
Quadruple therapy: |
-The Male and female patient had a negative PCR-test for SARS-CoV-2 after 7 days and 17 days respectively. -After receiving quadruple therapy, CT improvement was obtained after 10 days in male patient, and 8 days in female patient. |
-Only two cases. -No control group to show the relative efficacy of quadruple therapy. |
Abbreviation:
*IFN-ß: interferon-beta
†HCQ: hydroxychloroquine
‡IVIg: Intravenous Immunoglobulins
§ adjuvant drugs: interferon, arbidol, asmeton, eucalyptol limonene and penene entericsoft capsules and moxifloxacin.
¶SFJDC: Shufeng Jiedu Capsule
|| IFN-α2b: Interferon-alpha-2b.
|
Table2: Change of viral load, time to clinical improvement and reported side effects in thirteen studies. |
|||
|
Author |
PCR finding of change of viral load after LPV/r-based treatment |
Time to clinical improvement after LPV/r-based treatment |
Adverse events (percentage of patients) |
|
Cao et al. (2020) [20] |
Percentage of patients with undetectable level SARS-CoV-2 by PCR in both arm was similar: |
1.No significant difference when assessed by improvement in National Early Warning Score 2 (NEWS2) in intention-to-treat analysis.
2.Slightly shorter median time to obtain clinical improvement in treatment arm. Treatment arm requires 15 days and standard care requires 16 days (hazard ratio, 1.39; 95% CI, 1.00 to 1.91). But this was without statistical significance. |
Lymphopenia (8.0%) |
|
Hung et al. |
Earlier PCR test negative-conversion for SARS-CoV-2 in triple therapy group in all specimens (nasopharyngeal swab, posterior oropharyngeal swab saliva, throat swab and stool): [Triple therapy group] [Control group] The reported p-value is 0.0010. |
1.Earlier achievement of NEWS2 of 0 in triple therapy group (median is 4 days, IQR= 3 – 8 days) relative to control group (median is 8 days, 2.Earlier achievement of sequential organ failure assessment (SOFA) score of 0 in triple therapy group (median is 3.0 days; IQR:1.0-8.0 days) relative to control group (median is 8.0, IQR: 6.5 to 9.0 days). The p-value is 0.041. |
Nausea (33.9%) |
|
Righi et al. (2020) [15] |
PCR nasopharyngeal swab turned negative on day 6 after treatment with LPV/r associated with hydroxychloroquine. |
Fever ceased 2 days after LPV/r associated with hydroxychloroquine therapy. |
No data. |
|
Lim et al. (2020) [10] |
PCR turned negative after 8 days treatment with LPV/r. |
Fever ceased 6 days after treatment. |
Psychiatric symptoms such as depression, insomnia, and suicidal thoughts (100%) |
|
Fernandez-Ruiz |
No numerical data. |
6 patients were discharged between 8 to 23 days with adjustment of immunosuppressant dosage. 2 asymptomatic patients were on outpatient follow-up without any complication during treatment period. |
No data. |
|
Tang et al. (2020) [11] |
PCR turned negative after 8 days treatment with LPV/r. |
CT and laboratory test results showed improvements after 8 days of LPV/r. |
Not observable. |
|
Ye et al. (2020) [12] |
PCR test turned negative in LPV/r group earlier. |
1.Earlier return to normal body temperature in test group. 2.Lower abnormal proportion of White blood cells, lymphocytes, 3.Lymphocytes, haemoglobin, granulocytes and CRP gradually decreased throughout the tests. |
Liver biochemistry derangement. First measurement of liver biochemistry after treatment: [Treatment group] [Control group] Conclusion:Liver biochemistry derangement was not associated with side effects of medications. |
|
Wang et al. (2020) [13] |
4 patients were reported, their time taken to turn PCRnegative were 9,7,12 days and unreported in the 4th patient who was severely ill. |
1.Time taken to obtain CT improvement was 9 days, 9 days, 6 days and 11 days. 2.2 patients obtained improvement of arterial blood gas (ABG) parameter after 5 days and 11 days of treatment. 1 patient was with normal ABG throughout and the days taken for the 4th patient to obtain ABG improvement was unreported. |
No data. |
|
Liu et al. (2020) [14] |
In the 7 discharged patients, viral load decreased continuously during day 3 to 14.Negative conversion of PCR was demonstrated 3 days after treatment in 1 patient, and 7-14 days in the remaining 6 patients. 3 remaining patients were with respiratory complications and transferred to other hospital. Their PCR remained positive before they were transferred, despite they were receiving LPV/r. |
1.In the 7 discharged patients, radiograph improved continuously between day 6 and day 8. |
Hypokalaemia (70%) |
|
Han et al. (2020) [57] |
The patient obtained PCR test negative-conversion for SARS-CoV-2 on day 6 after treatment. |
CT improvement shown since day 6 and discharged on day 7. |
No data. |
|
Zhu et al. (2020) [29] |
On day 7, higher proportion of patients with undetectable viral load in arbidol group (50%) than LPV/r monotherapy group (23.5%). On day 14, higher proportion of patients with undetectable viral load in arbidol group (100%) than LPV/r monotherapy group (55.9%). Shorter duration of positive RNA test in arbidol group patients compared with LPV/r group (p<0.01). |
Higher percentage of patients with fever subsided within 7 days in arbidol group (88.2%) vs. LPV/r monotherapy group (81.3%). |
Rise of ALT (17.6%) |
|
Deng et al. (2020) [25] |
On day 7, higher proportion of patients obtained PCR test negative-conversion for SARS-CoV-2 in “LPV/r + Arbidol” combination group (75%) than LPV/r monotherapy group (35%), p<0.05. On day 14, higher proportion of patients obtained PCR test negative-conversion for SARS-CoV-2 in “LPV/r + Arbidol” combination group (94%) vs. LPV/r monotherapy group. (53%), p<0.05. Fewer patients showed PCR positive for stool SARS-CoV-2 in combination group (1 patient) vs. monotherapy group (3 patients). |
On day 7, more patients gained CT improvement in combination group (69%) than monotherapy group (29%), p<0.05. |
Elevated bilirubin (68.7%) |
|
Wang |
On day 7, the male patient obtained a negative conversion of PCR test for SARS-CoV-2. |
1.Patients were asymptomatic throughout the treatment period. 2.The male patient showed CT improvement 10 days after treatment. 3.The female patient showed CT improvement 8 days after treatment. |
Reported no adverse events |
Studies with LPV/r in treatment regimen were classified as LPV/r-based treatment (N=364), whether as monotherapy or in combination with other agent(s). Non-LPV/r based treatment (N=130) included standard care only (N=99), hydroxychloroquine (N=9), arbidol (N=21). Standard care comprised of supplemental oxygen, non-invasive and invasive ventilation, antibiotics, vasopressor support, renal replacement therapy and extracorporeal membrane oxygenation (ECMO). Among the thirteen studies, four studies had non LPV/r-based treatment (Cao et al, Fernandez et al, Ye et al. and Zhu et al). Cao et al. included standard care only; Fernandez et al. included hydroxychloroquine, Ye et al. and Zhu et al. included arbidol.
Figure 2 shows the number of patients with PCR negative-conversion for SARS-CoV-2 at different time intervals.
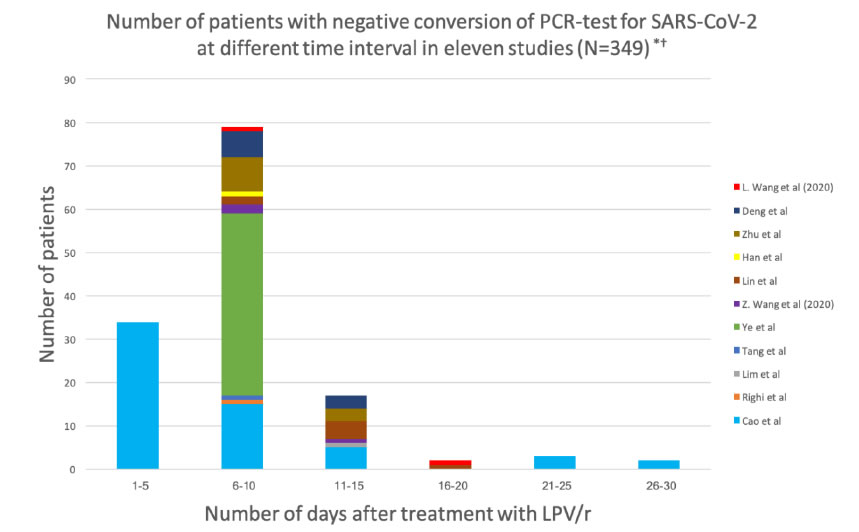
Figure 2. Number of days after LPV/r-based treatment and number of patients with negative conversion of PCR test for SARS-CoV-2 in eleven studies.
*The study by Fernandez et al. is excluded: authors did not provide data on negative conversion of PCR test for SARS-CoV-2.
†The study by Hung et al. is excluded: the data were in median and inter-quartile range (IQR).
Figure 3 shows the number of adverse events in LPV/r-based treatment group and non-LPV/r based treatment group in the thirteen studies.
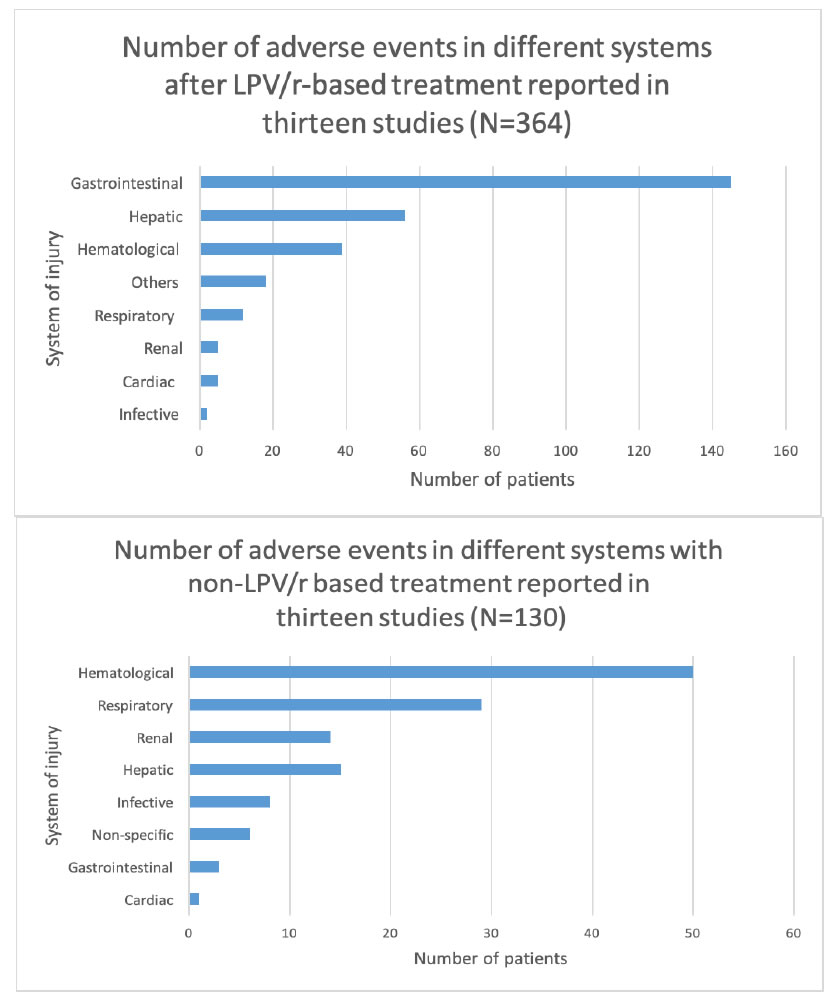
Figure 3. Total number of adverse events in different systems A) LPV/r-based treatment group reported in thirteen studies (N=364). B) non-LPV/r based treatment group in thirteen studies (N=130).
The distribution of adverse events in each system in respective treatment groups are as shown in Figures 4 and 5 respectively.
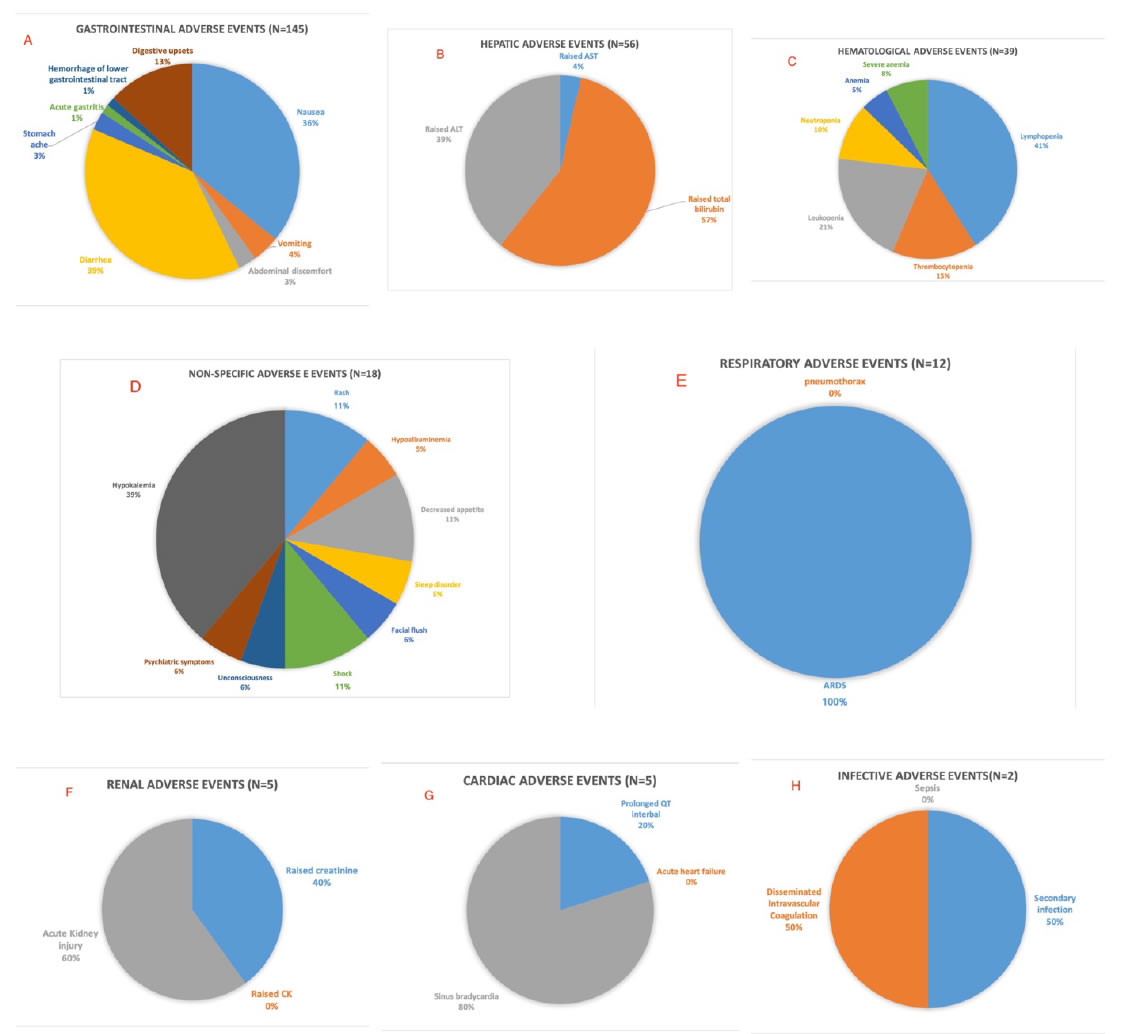
Figure 4. Distribution of adverse events in different systems in LPV/r-based treatment group in thirteen studies. (N=364).
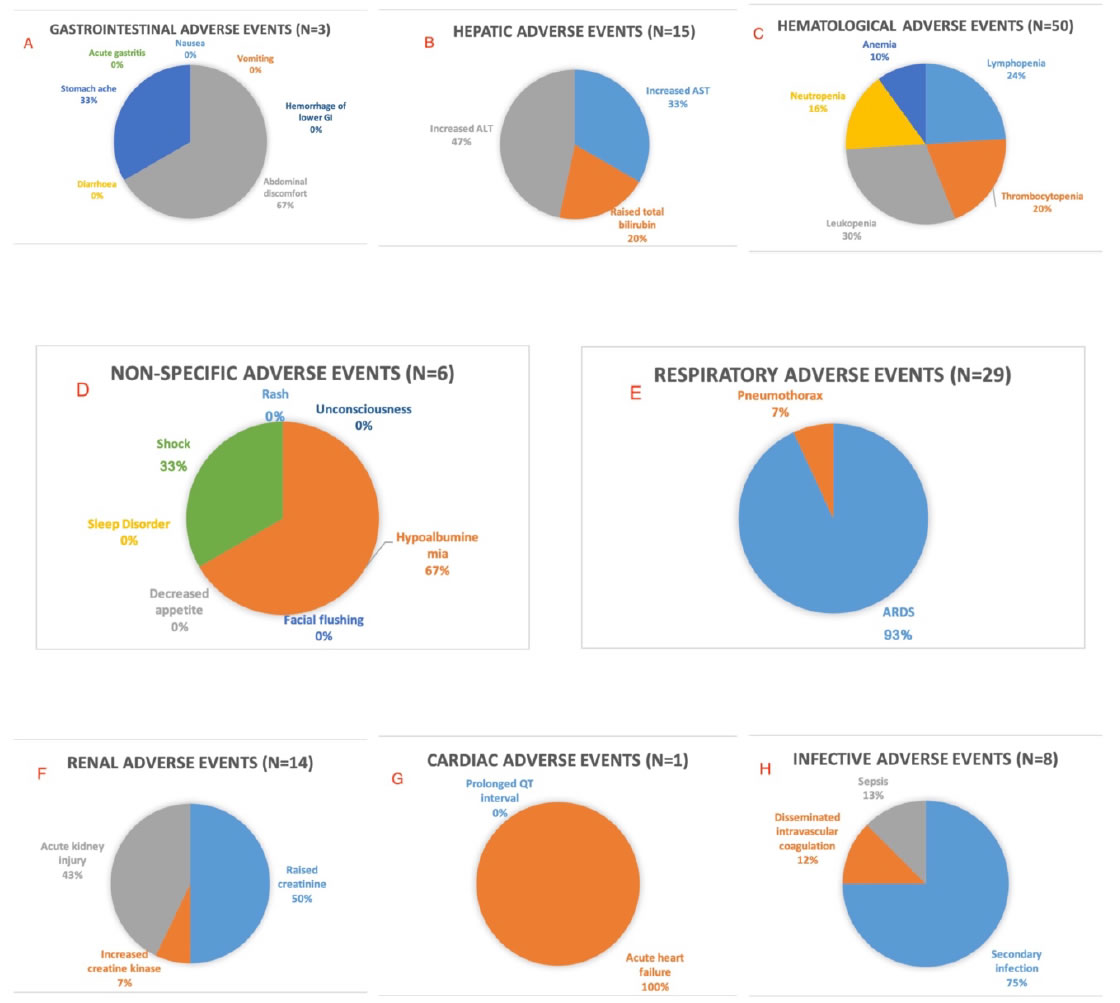
Figure 5. bution of adverse events in different systems in non-LPV/r based treatment group in thirteen studies (N=130).
Discussion
This is the first comprehensive review on the use of LPV/r in COVID-19 patients. The 13 eligible articles include two randomised clinical trials; others were case reports, retrospective cohort studies or case series. LPV/r and its combination with other medications have been reported, including arbidol, interferons, ribavirin, hydroxychloroquine/chloroquine, intravenous immunoglobulins, antibiotics, corticosteroid and Chinese medicine. Quality assessment was applied to the thirteen articles. However, evidence was insufficient to conduct a meta-analysis. Most articles are of low quality; the study designs were not consistent. The studies also showed discordance in conclusions. In spite of these limitations, this review provides updated information on the therapeutic effects of LPV/r in COVID-19 patients.LPV/r had been regarded as the key therapeutic for treatment of COVID-19 patients. Its effectiveness was first proven in in vitro experiment, and included in the third amendment of the Chinese CDC treatment guidelines for severe novel coronavirus infection. De wildeet al. (2014) reported that with mean EC50 of lopinavirranging from 6.6 to 17.1 μM, lopinavir showed effective anti-viral outcome against SARS-CoV, MERS-CoV and hCoV-229E in vitro [16]. However, this was not observed with ritonavir. Previously Chu et al. (2004) reported that a lower rate of development into acute respiratory distress or death was observed in SARS patients receiving LPV/r, when compared with the control group treated with ribavirin and corticosteroids [17]. Since SARS-CoV-2, SARS-CoV and MERS-CoV are all beta-coronaviruses, it has been hypothesized that LPV/r may be effective to combat SARS-CoV-2.Choy et al. (2020) reported that lopinavir (EC50 at 26.1 μM) reduces viral RNA copy of SARS-CoV-2 in vitro, but not with ritonavir alone [18]. This is consistent with the finding of De wildeet al. (2014) on the effect of LPV/r on SARS-CoV. However, ritonavir is used with lopinavir in 1:4 ratio because it increases lopinavir bioavailability in vivo, as seen in HIV patients [19]. In the thirteen selected studies (Figure 2), most supported the use of LPV/r as a viable anti-viral agent for SARS-CoV-2. Patients were responsive to treatment with negative-conversions of PCR testing for SARS-CoV-2 after 5 to 28 days of treatment, and clinical improvement was observable as early as 2 days as reported by Lim et al. [10]. For those responsive to treatment, the majority of them had a SARS-CoV-2 negative-conversion time between 6 days to 10 days.
However, there are discordances concerning the efficacy of LPV/r for COVID-19. Liu et al. reported three severe patients receiving LPV/r who showed no obvious clinical improvement; their clinical conditions worsened and were transferred to specialised care hospital [14]. In the randomised, controlled, open-label trial involving 199 severe COVID-19 patients with median National Early Warning Score 2 (NEWS2) of 5 reported by Cao et al. , the intention-to-treat analysis showed median time to clinical improvement was only shortened by 1 day compared to the control group with standard care [20]. (hazard ratio, 1.39, 95% CI, 1.00 to 1.91). There was a better outcome of 28-day mortality (treatment group:19.2% vs standard care group: 25%; difference: -5.8%; 95% CI, -17.3 to 5.7), shorter median days of stay in Intensive Care Units (treatment group:6 days vs standard care group:11 days; difference: -5 days; 95% CI, -9 to 0) and higher percentage of patients with clinical improvement at day 14 (treatment group: 45.5% vs standard care group:30.0%; difference:15.5 percentage points; 95% CI, 2.2. to 28.8) [20]. But none of these reached statistical significance. It was concluded that LPV/r added to standard supportive care was not associated with clinical improvement or mortality in severe COVID-19 patients. However, Hung et al. showed that LPV/r-based triple therapy is effective in a study of 127 non-severe COVID-19 patients with median NEWS2 of 2, by shortening the PCR negative-conversion time to within a week in more than half of the patients.Most of the other studies with promising effects of LPV/r recruited patients with non-severe SARS-CoV-2 infection.
Severe COVID patients are defined with the following characteristics by the Chinese CDC in their Seventh Amendment of COVID-19 guideline [21]:
1. Dyspnea and tachypnea ≥ 30 breaths per minute
2. Blood oxygen saturation ≤ 93% when not in exertion
3. PaO2/FiO2 ≤ 300 mmHg.
4. Signs of respiratory failure, shock, multi-organ failure or need of mechanical ventilation and ICU admission.
In view of the insufficient clinical data to date, additional larger scale double-blinded randomized controlled trials, with classification of patient’s clinical status into severe and non-severe type, should be carried out before LPV/r can be adopted in international guidelines. Currently, it is advisable for physicians to classify the severity of COVID-19 patients. It is likely that LPV/r may be effective in reducing viral load in non-severe COVID-19 patients, but its benefits remain questionable in severe patients. Severe COVID-19 is associated with immunopathological damages such as diffuse alveolar damage with hyaline membrane formation [22]. This may be caused by cytokine storms or inflammatory processes [23]. Since 19% of patients have the severe form[24], patients should be classified soon after admission. Once recognised, they should be treated to minimize the cytokine storm. Steroid was used as adjuvant therapy in some studies [12,14,25-27]. This is debatable because Auyeunget al. (2005) showed that use of steroid was associated with adverse outcomes in SARS [28]. Combining LPV/r with other drugs seems to be an effective modality of treatment. Zhu et al. reported that arbidol monotherapy achieved better reduction of viral load to an undetectable level than LPV/r monotherapy on day 7 (arbidol: 50% vs LPV/r:23.5%) and on day 14 (arbidol:100% vs 54.9%) [29]. Deng et al. reported that an even higher proportion of negative-conversion of PCR test for SARS-CoV-2 could be achieved with “arbidol and LPV/r” combination therapy (Day 7: 75%, Day 14: 94%)than LPV/r monotherapy (Day 7:35%, Day 14: 53%) [25]. Hung et al. showed that an earlier PCR negative-conversion was also obtained in LPV/r-based triple therapy (median=8 days, IQR=6-12 days) than control group (median=13 days, IQR=8-15 days), p-value=0.0010. Combinations with remdesivir and hydroxychloroquine should also be studied together with LPV/r to explore the more effective combinations, they being inhibitors of SARS-CoV-2 through mediation of viral polymerase and the proofreading exoribonuclease [30,31]. Clinical usage of LPV/r requires extra care in special populations. Fernandez et al. reported 18 post-organ transplant patients on immunosuppressants. Therapeutic regimens and dosages were adjusted when LPV/r was initiated [26]. Calcineurin and mammalian target of rapamycin (mTOR) inhibitors were stopped, and prednisolone was reduced by 50% in these patients. The serum trough concentrations of LPV/r were obtained after 48-72 hours, with close monitoring for adjustment of dosage. The dosage of mycophenolate mofetil/mycophenolic acid (MMF/MPA) was decreased in patients receiving LPV/r. Similarly in the studies by Fan et al. and Zhang et al. on renal transplant recipients, patients were given reduced dosage of immunosuppressants and methylprednisolone [32,33]. When patients developed severe graft rejection, consideration of alternative antiviral and continuation of corticosteroid at reduced dose has been suggested [34]. Another group for special consideration are cancer patients due to drug interaction with CYP3A4, a common pathway for chemotherapeutic agents. Liang et al. showedthat cancer patients with COVID-19 were associated with higher risks of severe events compared to patients without cancers [35]. This might be due to the leukopenia and lymphopenia commonly found among COVID-19 patients [36], leading to a higher risk of super-infections. In addition, the dosage of some chemotherapeutic agents may require readjustment [37] such as docetaxel [38] anderlotinib [39]. Therefore, in managing drug interactions between chemotherapeutic and antiviral agents, it is advised to consider the following [35]:
1. Intentional postponing of adjuvant chemotherapy or elective surgery for stable cancer;
2. Strong personal protection provisions for cancer patients and survivors;
3. More intensive surveillance or treatment when cancer patients are infected with SARS-CoV-2, especially in older patients and those with comorbidities.
Another patient group with immunocompromised state are patients on hemodialysis. Hemodialysis predisposes to chronic immunocompromised state due to disorders of B cell and T cell function [40,41]. T cells play a vital role for patients’ recovery from other beta-coronavirus infection[42-44]. But lymphopeniais commonly observed in hemodialysis patients [45]. No dose adjustment is deemednecessary in the treatment of hemodialysis patients with COVID-19, probably due to the liver clearance and the high protein-binding capacity of LPV/r [26].The effects of COVID-19 on pregnancy are noteworthy. Li et al. summarized the outcomes of 55 pregnant COVID-19 women and 46 neonates: vertical transmission to neonates was not observed[46,47].This was further confirmed by Chen et al. [47]: 3 out of 4 infants tested negative for SARS-CoV-2 (consent was not obtained for the forth infant).Use of LPV/r in pregnancy is safe, as documented by a study of population-based surveillance in HIV-positive pregnancies. It found no increase in the risk of foetal anomalies, preterm birth nor low-birth weight infants [48]. This was further confirmed in pregnant mothers with COVID-19. However, it is advisable to have close surveillance of both the mothers and the neonates. In case of maternal hypoxia due to SARS-CoV-2 infection, there would be an increase of endothelin-1 and hypoxia-inducible factor, impairing placental perfusion to the fetus [49]. Therefore, at least one ultrasound after maternal recovery is recommended to monitor the potential intra-uterine growth retardation, which was observed in approximately 10% of COVID-19 pregnancies. However, SARS-CoV-2 infection during pregnancy was not found to be associated with an increased risk of spontaneous abortion and preterm birth [50]. Chen et al. did a study involving 118 pregnancy women and found that SARS-CoV-2 infection during pregnancy did not increase the risk of severe disease among pregnancy women. The risk is only half of that in the general population [51]. Pregnant women are at higher risks of hypercoagulability than the general population. Physicians should monitor possible thromboembolic events in severe COVID-19 pregnancy, because the incidence of venous thromboembolism is more than 30% in severe COVID-19 patients [52]. The side effects of LPV/r need to be monitored. These include nausea, vomiting, gastrointestinal disturbances, pancreatitis, hepatotoxicity, QT interval prolongation, PR interval prolongation, and metabolic disturbances [51]. In the 13 studies (Figures 3 and 4), of the 364 COVID-19 patients receiving LPV-r based treatment, 145 patients (39.8%) had gastrointestinal adverse effects after LPV/r treatment. Hepatic injury was observed in 56 patients (15.4%). 12 patients (3.30%) had respiratory failure. Prolongation of QT interval was only observed in 1 patient. Haematological alteration was observed in 39 patients (10.7%). Eight patients (2.20%) showed leukopenia. Granulocytes colony stimulating factor (GCSF)was prescribed whichprevented complications in 3 patients [29]. Other side effects such as metabolic disturbances and PR interval prolongation have not been reported. Because of the possible side effects, patients should be closely monitored. In digestive tract adverse effects, hydration status and electrolytes should be monitored. With severe nausea and vomiting, use of anti-emetics or stopping medication may be possible choices. However, the use of 5-HT3 receptor antagonists and neurokinin-1 receptor antagonists shall be cautious due to their risk of QT prolongation and prolonged serum concentration [53]. Liver biochemistry derangement may be due to the following causes: LPV/r induced, SARS-CoV-2 related or immune-mediated inflammation such as cytokine storm. Liver biochemistry usually returns to normal without specific treatment in mild COVID-19 [54]. Ye et al. reported liver enzyme elevations in both LPV/r-based and non LPV/r-based treatment groups, and it was found to be unrelated to treatment. However, with extensive hepatic damage orpre-existing liver diseases, close monitoring of liver biochemistry should be considered [55]. In immune-mediated inflammation, the use of glucocorticoid is unclear.
Prolonged QT interval and ventricular arrhythmia are two serious adverse effects of LPV/r.The Canadian Heart Rhythm Society has published guidelines on minimizing the risk [56]:
1. Discontinue unnecessary medications that prolong QT interval.
2. Identify low-risk outpatients who do not need further testing (no history of prolonged QT, unexplained syncope or family history of premature sudden cardiac death, no medications
which may prolong the QT interval, and/or prior known
normal QTc.
3. Performing baseline testing in hospitalized and high-risk patients. If the QTc is markedly prolonged, drugs which further prolong QTc should be avoided. Expert consultation may permit administration with mitigating precautions.
Conclusion
With the evidence to date, the review shows that LPV/r may be effective for treating non-severe COVID-19 patients, while only limited benefits are observed in severe COVID-19 patients. Clinical classification and close monitoring of drug dosage and treatment progress are recommended for special populations. Further research on LPV/r, precluding in combination with other drugs, are required to confirm its use for COVID-19 patients.
Evidence before This Study
Published studies on electronic databases such as Pubmed, Embase and Medline on the use of LPV/r in the treatment of COVID-19 patients are conflicting. Previously only an inconclusive rapid review was done. No systematic review nor meta-analysis have been performed to date to evaluate the results. The real therapeutic effect of LPV/r is debatable. A systematic search on the three electronic databases was done on 9 May, 2020 and outputs were gathered for a systematic review of the therapeutic outcome, adverse events and clinical management of special populations. Search terms used included: Lopinavir, SARS-CoV-2, COVID-19. Full peer-reviewed articles that are written in English, published between 2019 and 2020, accessible on the three databases are included in this systematic review.Items without therapeutic data were eliminated.
Added Value of This Study
The review selected thirteen articles with primary therapeutic data to look at the therapeutic effect of LPV/r, number of adverse events, distribution of adverse events in different systems and the precautions in prescribing LPV/r in special populations with COVID-19. Most studies were of low evidence value, with potential experimental bias. Their outcome measures varied. It is likely that LPV/r is effective in treating non-severe COVID-19 patients, but only limited benefits are observed in severe COVID-19 patients. Clinical classification of patients according to the severity of COVID-19 infections should be carried out for a better treatment plan.
Implications of All the Available Evidence
LPV/r may be considered in non-severe COVID-19 patients. Further research of LPV/r, preferably in combination with other antiviral agents, in severe COVID-19 patients is required for more effective treatment.
Contributions
Literature search was done by ZY, KLS and CLL. Searches screening, and article review was done by ZY, KLS and CLL. Study designs were done by ZY,KLS and CLL. Data extraction and analysis was done by ZY and CLL. Data interpretation was done by ZY and CLL. Manuscript writing was done by ZY, KLS and CLL.
Declaration of interests
Prof. Ching-Lung Lai has given sponsored lectures on hepatitis C for Abbvie Inc.
Ethical approval
No ethical approval is required since the whole review is based on published data on readily-accessible databases.
Acknowledgement
None.
Funding
None.
References
- Huang C, Wang Y, Li X,Lili Ren, Jianping Zhao,et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395: 497-506.
- Li Q, Guan X, Wu P,Xiaoye Wang, Lei Zhou, et al. (2020) Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N Engl J Med 382: 1199-1207. [crossref]
- Sanche S, Lin YT, Xu C, Romero-Severson E, Hengartner N, et al. (2020) High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus 2. Emerg Infect Dis26. [crossref]
- WHO. WHO announces COVID-19 outbreak a pandemic. 2020.
- WHO. Coronavirus disease (COVID-19) Situation Report– 111. 2020 May 11.
- Hassan SA, Sheikh FN, Jamal S, Ezeh JK, Akhtar A (2020) Coronavirus (COVID-19): A Review of Clinical Features, Diagnosis, and Treatment. Cureus12. [crossref]
- Chinese Centre for Disease Control and Prevention. Chinese CDC "novel coronavirus infection treatment guideline third amendment". 2020.
- Yao TT, Qian JD, Zhu WY, Wang Y, Wang GQ (2020) A systematic review of lopinavir therapy for SARS coronavirus and MERS coronavirus-A possible reference for coronavirus disease-19 treatment option. J Med Virol92: 556-563. [crossref]
- Dorward J, Gbinigie K (2020) Lopinavir/ritonavir: A rapid review of effectiveness in COVID-19.
- Lim J, Jeon S, Shin HY, Jung KM, Seong YM, et al. (2020) Case of the Index Patient Who Caused Tertiary Transmission of COVID-19 Infection in Korea: the Application of Lopinavir/Ritonavir for the Treatment of COVID-19 Infected Pneumonia Monitored by Quantitative RT-PCR. J Korean Med Sci35. [crossref]
- Tang B, Li S, Xiong Y,Ming Tian, Jianbin Yu, et al. (2020) Coronavirus Disease 2019 (COVID-19) Pneumonia in a Hemodialysis Patient. Kidney Med. [crossref]
- Ye XT, Luo YL, Xia SC,Sun QF, Ding JG, et al. (2020) Clinical efficacy of lopinavir/ritonavir in the treatment of Coronavirus disease 2019. Eur Rev Med Pharmacol Sci24: 3390-3396.
- Wang Z, Chen X, Lu Y, Chen F, Zhang W (2020) Clinical characteristics and therapeutic procedure for four cases with 2019 novel coronavirus pneumonia receiving combined Chinese and Western medicine treatment. Biosci Trends14: 64-68. [crossref]
- Liu F, Xu A, Zhang Y,Weiling Xuan, Tingbo Yan, et al.(2020)Patients of COVID-19 may benefit from sustained lopinavir-combined regimen and the increase of eosinophil may predict the outcome of COVID-19 progression. Int J Infect Dis 95: 83-191.
- Righi G, Del Popolo G (2020) COVID-19 tsunami: the first case of a spinal cord injury patient in Italy. Spinal Cord Ser Cases6.
- De Wilde AH, Jochmans D, Posthuma CC, Zevenhoven-Dobbe JC, Stefan van Nieuwkoop,et al. (2014) Screening of an FDA-approved compound library identifies four small-molecule inhibitors of Middle East respiratory syndrome coronavirus replication in cell culture. Antimicrob Agents Chemother58: 4875-4884. [crossref]
- Chu CM, Cheng VC, Hung IF,Wong MML,Chan KH, et al. (2004) Role of lopinavir/ritonavir in the treatment of SARS: initial virological and clinical findings. Thorax59: 252-256. [crossref]
- Choy KT, Wong AY, Kaewpreedee P,Sin Fun Sia, Dongdong Chen, et al. (2020) Remdesivir, lopinavir, emetine, and homoharringtonine inhibit SARS-CoV-2 replication in vitro. Antiviral Res 178. [crossref]
- Kempf DJ, Marsh KC, Kumar G,A D Rodrigues,Denissen JF, et al. (1997) Pharmacokinetic enhancement of inhibitors of the human immunodeficiency virus protease by coadministration with ritonavir. Antimicrob Agents Chemother41: 654-660. [crossref]
- Cao B, Wang Y, Wen D,Wen Liu,Jingli Wang, et al. (2020) A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19. N Engl J Med382: 1787-1799.
- Chinese Centre for Disease Control and Prevention. Novel coronavirus infection treatment guideline seventh edition 2020.
- Xu Z, Shi L, Wang Y, Jiyuan Zhang, Lei Huang,et al. (2020) Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med8: 420-422. [crossref]
- Mehta P, McAuley DF, Brown M,Emilie Sanchez, Rachel S Tattersall, et al. (2020) COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet395: 1033-1034. [crossref]
- Wu Z, McGoogan JM (2020) Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA.
- Deng L, Li C, Zeng Q,Xi Liu, Xinghua Li, et al. (2020)Arbidol combined with LPV/r versus LPV/r alone against Corona Virus Disease 2019: A retrospective cohort study. J Infect 81.
- Fernandez-Ruiz M, Andres A, Loinaz C, Juan F Delgado, Francisco López-Medrano,et al. (2020) COVID-19 in solid organ transplant recipients: a single-center case series from Spain. Am J Transplant. [crossref]
- Hung IFN LK, Cheung LK,Tso EYK, Raymond Liu, Tom Wai-Hin Chung, et al, (2020) Triple combination of interferon beta-1b, lopinavir–ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: an open-label, randomised, phase 2 trial.Lancet.395:1695-1704. [crossref]
- Auyeung TW, Lee JS, Lai WK,Chun HC, Lee KH, et al. (2005) The use of corticosteroid as treatment in SARS was associated with adverse outcomes: a retrospective cohort study. J Infect51: 98-102. [crossref]
- Zhu Z, Lu Z, Xu T,Cong Chen, Gang Yang, et al. (2020)Arbidol monotherapy is superior to lopinavir/ritonavir in treating COVID-19. J Infect 81. [crossref]
- Wang M, Cao R, Zhang L,Xinglou Yang, Jia Liu, et al. (2020) Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res30: 269-271. [crossref]
- Agostini ML, Andres EL, Sims AC,Rachel LG, Timothy PS, et al. (2018) Coronavirus Susceptibility to the Antiviral Remdesivir (GS-5734) Is Mediated by the Viral Polymerase and the Proofreading Exoribonuclease. mBio.
- Zhu L, Xu X, Ma K,Yang, Junling,GuanHanxiong, et al. (2020) Successful recovery of COVID-19 pneumonia in a renal transplant recipient with long-term immunosuppression. Am J Transplant .
- Guillen E, Pineiro GJ, Revuelta I,Rodriguez D, Marta Bodro, et al. (2020)Case report of COVID-19 in a kidney transplant recipient: Does immunosuppression alter the clinical presentation? Am J Transplant.
- Bartiromo M, Borchi B, Botta A,Bagalà A, Gianmarco L, et al. (2020) Threatening drug-drug interaction in a kidney transplant patient with Coronavirus Disease 2019 (COVID-19). Transpl Infect Dis. [crossref]
- Liang W, Guan W, Chen R,Wang W, Jianfu L, et al. (2020) Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol21: 335-337. [crossref]
- Guan WJ, Ni ZY, Hu Y,en-hua Liang, Chun-quan Ou, et al. (2020) Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med382: 1708-1720. [crossref]
- Rudek MA, Moore PC, Mitsuyasu RT,Bruce J Dezube, David Aboulafia, et al. (2014)A phase 1/pharmacokinetic study of sunitinib in combination with highly active antiretroviral therapy in human immunodeficiency virus-positive patients with cancer: AIDS Malignancy Consortium trial AMC 061. Cancer; 120: 1194-1202. [crossref]
- Oostendorp RL, Huitema A, Rosing H,Robert SJ, Heine RT et al. (2009) Coadministration of ritonavir strongly enhances the apparent oral bioavailability of docetaxel in patients with solid tumors. Clin Cancer Res; 15: 4228-4233.
- Pillai VC, Venkataramanan R, Parise RA,Susan MC, Roberto G, et al. (2013) Ritonavir and efavirenz significantly alter the metabolism of erlotinib–an observation in primary cultures of human hepatocytes that is relevant to HIV patients with cancer. Drug Metab Dispos41: 1843-1851. [crossref]
- Borges A, Borges M, Fernandes J,Henrique N, SameiroFM, et al. (2011)Apoptosis of peripheral CD4(+) T-lymphocytes in end-stage renal disease patients under hemodialysis and rhEPO therapies. Ren Fail33: 138-143. [crossref]
- Freitas GRR, da Luz Fernandes M, Agena F, Omar Jaluul, Sérgio CS et al. (2019)Aging and End Stage Renal Disease Cause A Decrease in Absolute Circulating Lymphocyte Counts with A Shift to A Memory Profile and Diverge in Treg Population. Aging Dis 10: 49-61. [crossref]
- Channappanavar R, Zhao J, Perlman S (2014) T cell-mediated immune response to respiratory coronaviruses. Immunol Res59: 118-128. [crossref]
- Janice Oh HL, Ken-En Gan S, Bertoletti A, Tan YJ, Yee-Joo Tan (2012) Understanding the T cell immune response in SARS coronavirus infection. Emerg Microbes Infect1. [crossref]
- Liu WJ, Zhao M, Liu K,KunXu, GaryWong, et al. (2017)T-cell immunity of SARS-CoV: Implications for vaccine development against MERS-CoV. Antiviral Res137: 82-92.
- Meisner M, Lohs T, Huettemann E, Schmidt J, Hueller M, et al. (2001)The plasma elimination rate and urinary secretion of procalcitonin in patients with normal and impaired renal function. Eur J Anaesthesiol18: 79-87. [crossref]
- Li Y, Zhao R, Zheng S,Xu Chen, Jinxi Wanget al. (2020) Lack of Vertical Transmission of Severe Acute Respiratory Syndrome Coronavirus 2, China. Emerg Infect Dis. [crossref]
- Chen Y, Peng H, Wang L,Yin Zhao, Lingkong Zeng et al. (2020) Infants Born to Mothers With a New Coronavirus (COVID-19). Front Pediatr8. [crossref]
- Tookey PA, Thorne C, van Wyk J, Norton M (2016) Maternal and foetal outcomes among 4118 women with HIV infection treated with lopinavir/ritonavir during pregnancy: analysis of population-based surveillance data from the national study of HIV in pregnancy and childhood in the United Kingdom and Ireland. BMC Infect Dis16. [crossref]
- Dashraath P, Wong JLJ, Lim MXK,Mahesh Choolani, Citra Mattar, et al. (2020) Coronavirus disease 2019 (COVID-19) pandemic and pregnancy. Am J Obstet Gynecol 222.
- Yan J, Guo J, Fan C,Yuanzhen Zhang, Liona C. Poon,et al. (2020) Coronavirus disease 2019 (COVID-19) in pregnant women: A report based on 116 cases. Am J Obstet Gynecol.
- Chen L, Li Q, Zheng D,Hai Jiang, Yuan Wei, et al. (2020) Clinical Characteristics of Pregnant Women with Covid-19 in Wuhan, China. N Engl J Med. [crossref]
- Klok FA, Kruip M, van der Meer NJM,Arbous MS, Gommers DAMPJ, et al. (2020) Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res191: 145-147.
- Zheng XW, Tao G, Zhang YW, Yang GN, Huang P (2020)[Drug interaction monitoring of lopinavir / ritonavir in COVID-19 patients with cancer]. Zhonghua Nei Ke Za Zhi59: 400-404. [crossref]
- Fan Z, Chen L, Li J,Xin Cheng, et al. (2020) Clinical Features of COVID-19-Related Liver Damage. Clin Gastroenterol Hepatolc18.
- Zhang C, Shi L, Wang FS (2020). Liver injury in COVID-19: management and challenges. Lancet Gastroenterol Hepatol5: 428-430. [crossref]
- Sapp JL, Alqarawi W, MacIntyre CJ,Rafik Tadros, Christian Steinberg, et al. (2020) Guidance On Minimizing Risk of Drug-Induced Ventricular Arrhythmia During Treatment of COVID-19: A Statement from the Canadian Heart Rhythm Society. Can J Cardiol36: 948-951. [crossref]
- Han W, Quan B, Guo Y,Jun Zhang, Yong Lu, et al.(2020) The course of clinical diagnosis and treatment of a case infected with coronavirus disease 2019. J Med Virol92: 461-463. [crossref]
- Wang L, Xu X, Ruan J, Lin S, Jiang J, et al. (2020)Quadruple therapy for asymptomatic COVID-19 infection patients. Expert Rev Anti Infect Ther 3:1-8. [crossref]
Appendix
|
Appendix table. List of excluded papers |
||||
|
No.# |
Authors |
Title |
Covid-19 |
Reason for exclusion |
|
1 |
Khot WY, Nadkar MY. The 2019 Novel Coronavirus Outbreak – A Global Threat. J Assoc Physicians India. 2020;68:67-71. |
The 2019 Novel Coronavirus Outbreak – A Global Threat |
Yes |
No details on LPV/r therapeutics |
|
2 |
Ahmad A, Rehman MU, Alkharfy KM. An alternative approach to minimize the risk of coronavirus (Covid-19) and similar infections. Eur Rev Med Pharmacol Sci. 2020;24:4030-4. |
An alternative approach to minimize the risk of coronavirus (Covid-19) and similar infections |
Yes |
No details on LPV/r therapeutics |
|
3 |
Khan Z, Karatas Y, Rahman H. Anti COVID-19 Drugs: Need for More Clinical Evidence and Global Action. Adv Ther. 2020. Apr 29. |
Anti COVID-19 Drugs: Need for More Clinical Evidence and Global Action |
Yes |
Review |
|
4 |
Yousefifard M, Zali A, Mohamed Ali K, Madani Neishaboori A, Zarghi A, Hosseini M, et al. Antiviral therapy in management of COVID-19: a systematic review on current evidence. Arch Acad Emerg Med. 2020;8:e45. |
Antiviral therapy in management of COVID-19: a systematic review on current evidence. |
Yes |
Review |
|
5 |
Simsek Yavuz S, Unal S. Antiviral treatment of COVID-19. Turk J Med Sci. 2020;50:611-9. |
Antiviral treatment of COVID-19 |
Yes |
Review |
|
6 |
Vanden Eynde JJ. COVID-19: A Brief Overview of the Discovery Clinical Trial. Pharmaceuticals (Basel, Switzerland) 2020 Apr 10. |
A Brief Overview of the Discovery Clinical Trial |
Yes |
Review |
|
7 |
Liu YJ, Yang YL, Xu Y. [What we learned from SARS may provide important insights into understanding and management of coronavirus disease 2019]. Zhonghua Jie He He Hu Xi Za Zhi 2020 Apr 12;43:339-344. |
[What we learned from SARS may provide important insights into understanding and management of coronavirus disease 2019] |
Yes |
Review |
|
8 |
Rubin EJ, Baden LR, Morrissey S. Audio Interview: New Research on Possible Treatments for Covid-19. N Engl J Med. 2020;382:e30. |
Audio Interview: New Research on Possible Treatments for Covid-19 |
Yes |
Review |
|
9 |
Lim J, Jeon S, Shin HY, Kim MJ, Seong YM, Lee WJ, et al. The Author’s Response: Case of the Index Patient Who Caused Tertiary Transmission of Coronavirus Disease 2019 in Korea: the Application of Lopinavir/Ritonavir for the Treatment of COVID-19 Pneumonia Monitored by Quantitative RT-PCR. J Korean Med Sci. 2020;35:e89. |
Author’s Response: Case of the Index Patient Who Caused Tertiary Transmission of Coronavirus Disease 2019 in Korea: the Application of Lopinavir/Ritonavir for the Treatment of COVID-19 Pneumonia Monitored by Quantitative RT-PCR |
Yes |
No details on LPV/r therapeutics |
|
10 |
Mothay D, Ramesh KV. Binding site analysis of potential protease inhibitors of COVID-19 using AutoDock. Virusdisease. 2020 2:1-6. |
Binding site analysis of potential protease inhibitors of COVID-19 using AutoDock |
Yes |
No details on LPV/r therapeutics |
|
11 |
McKee DL, Sternberg A, Stange U, Laufer S, Naujokat C. Candidate drugs against SARS-CoV-2 and COVID-19. Pharmacol Res. 2020:104859. |
Candidate drugs against SARS-CoV-2 and COVID-19 |
Yes |
Review |
|
12 |
Inciardi RM, Lupi L, Zaccone G, Italia L, Raffo M, Tomasoni D, et al. Cardiac Involvement in a Patient With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020. Mar 27. DOI: 10.1001/jamacardio.2020.1096 |
Cardiac Involvement in a Patient With Coronavirus Disease 2019 (COVID-19) |
Yes |
No details on LPV/r therapeutics |
|
13 |
Naksuk N, Lazar S, Peeraphatdit TB. Cardiac safety of off-label COVID-19 drug therapy: a review and proposed monitoring protocol. Eur Heart J Acute Cardiovasc Care. 2020:2048872620922784. |
Cardiac safety of off-label COVID-19 drug therapy: a review and proposed monitoring protocol |
Yes |
No details on LPV/r therapeutics |
|
14 |
Kakodkar P, Kaka N, Baig MN. A Comprehensive Literature Review on the Clinical Presentation, and Management of the Pandemic Coronavirus Disease 2019 (COVID-19). Cureus 2020 Apr 06;12:1. |
Comprehensive Literature Review on the Clinical Presentation, and Management of the Pandemic Coronavirus Disease 2019 (COVID-19) |
Yes |
Review |
|
15 |
Qiu H, Wu J, Hong L, Luo Y, Song Q, Chen D. Clinical and epidemiological features of 36 children with coronavirus disease 2019 (COVID-19) in Zhejiang, China: an observational cohort study. Lancet Infect Dis. 2020. Mar 25. |
Clinical and epidemiological features of 36 children with coronavirus disease 2019 (COVID-19) in Zhejiang, China: an observational cohort study |
Yes |
No details on LPV/r therapeutics |
|
16 |
Allameh S.F. All about COVID-19 in brief. New Microbes and New Infections. 2020;35:no pagination. |
All about COVID-19 in brief |
Yes |
No details on LPV/r therapeutics |
|
17 |
Du B, Qiu HB, Zhan X, Wang YS, Kang HYJ, Li XY, et al. [Pharmacotherapeutics for the new coronavirus pneumonia]. Zhonghua Jie He He Hu Xi Za Zhi 2020 Mar 12;43:173-176. |
[Pharmacotherapeutics for the new coronavirus pneumonia] |
Yes |
Review |
|
18 |
Liu K, Chen Y, Lin R, Han K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J Infect. 2020. Mar 27. |
Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients |
Yes |
No details on LPV/r therapeutics |
|
19 |
Fan Z, Chen L, Li J, Cheng X, Yang J, Tian C, et al. Clinical Features of COVID-19-Related Liver Damage. Clin Gastroenterol Hepatol. 2020. Apr 10. |
Clinical Features of COVID-19-Related Liver Damage |
Yes |
No details on LPV/r therapeutics |
|
20 |
Rosa SGV, Santos WC. Clinical trials on drug repositioning for COVID-19 treatment. Rev Panam Salud Publica. 2020;44:e40. |
Clinical trials on drug repositioning for COVID-19 treatment |
Yes |
Review |
|
21 |
Martinez MA. Compounds with Therapeutic Potential against Novel Respiratory 2019 Coronavirus. Antimicrob Agents Chemother. 2020;Apr 21. |
Compounds with Therapeutic Potential against Novel Respiratory 2019 Coronavirus |
Yes |
Review |
|
22 |
Lv DF, Ying QM, Weng YS, Shen CB, Chu JG, Kong JP, et al. Dynamic change process of target genes by RT-PCR testing of SARS-Cov-2 during the course of a Coronavirus Disease 2019 patient. Clin Chim Acta. 2020;506:172-5. |
Dynamic change process of target genes by RT-PCR testing of SARS-Cov-2 during the course of a Coronavirus Disease 2019 patient |
Yes |
No details on LPV/r therapeutics |
|
23 |
Muralidharan N, Sakthivel R, Velmurugan D, Gromiha MM. Computational studies of drug repurposing and synergism of lopinavir, oseltamivir and ritonavir binding with SARS-CoV-2 protease against COVID-19. J Biomol Struct Dyn. 2020; 16:1-6. |
Computational studies of drug repurposing and synergism of lopinavir, oseltamivir and ritonavir binding with SARS-CoV-2 protease against COVID-19 |
Yes |
No details on LPV/r therapeutics |
|
24 |
Song J, Kang S, Choi SW, Seo KW, Lee S, So MW, et al. Coronavirus Disease 19 (COVID-19) complicated with pneumonia in a patient with rheumatoid arthritis receiving conventional disease-modifying antirheumatic drugs. Rheumatol Int. 2020;40:991-5. |
Coronavirus Disease 19 (COVID-19) complicated with pneumonia in a patient with rheumatoid arthritis receiving conventional disease-modifying antirheumatic drugs |
Yes |
No details on LPV/r therapeutics |
|
25 |
Wang M, Zhou Y, Zong Z, Liang Z, Cao Y, Tang H, et al. A precision medicine approach to managing 2019 novel coronavirus pneumonia. Precis Clin Med. 2020;3:14-21. |
A precision medicine approach to managing 2019 novel coronavirus pneumonia |
Yes |
No details on LPV/r therapeutics |
|
26 |
McCreary EK, Pogue JM. Coronavirus Disease 2019 Treatment: A Review of Early and Emerging Options. Open Forum Infect Dis. 2020;7:ofaa105. |
Coronavirus Disease 2019 Treatment: A Review of Early and Emerging Options |
Yes |
Review |
|
27 |
Yuan J, Zou R, Zeng L, Kou S, Lan J, Li X, et al. The correlation between viral clearance and biochemical outcomes of 94 COVID-19 infected discharged patients. Inflamm Res. 2020;69:599-606. |
The correlation between viral clearance and biochemical outcomes of 94 COVID-19 infected discharged patients |
Yes |
No details on LPV/r therapeutics |
|
28 |
Han W, Quan B, Guo Y, Zhang J, Lu Y, Feng G, et al. The course of clinical diagnosis and treatment of a case infected with coronavirus disease 2019. J Med Virol. 2020;92:461-3. |
The course of clinical diagnosis and treatment of a case infected with coronavirus disease 2019 |
Yes |
No details on LPV/r therapeutics |
|
29 |
Guzik TJ, Mohiddin SA, Dimarco A, Patel V, Savvatis K, Marelli-Berg FM, et al. COVID-19 and the cardiovascular system: implications for risk assessment, diagnosis, and treatment options. Cardiovasc Res. 2020. Apr 30. |
COVID-19 and the cardiovascular system: implications for risk assessment, diagnosis, and treatment option |
Yes |
Review |
|
30 |
Sankar J, Dhochak N, Kabra SK, Lodha R. COVID-19 in Children: Clinical Approach and Management. Indian J Pediatr. 2020. Apr 27. |
COVID-19 in Children: Clinical Approach and Management |
Yes |
Review |
|
31 |
Ma J, Xia P, Zhou Y, Liu Z, Zhou X, Wang J, et al. Potential effect of blood purification therapy in reducing cytokine storm as a late complication of critically ill COVID-19. Clin Immunol. 2020;214:108408. |
Potential effect of blood purification therapy in reducing cytokine storm as a late complication of critically ill COVID-19 |
Yes |
No details on LPV/r therapeutics |
|
32 |
Bleasel MD, Peterson GM. Emetine, Ipecac, Ipecac Alkaloids and Analogues as Potential Antiviral Agents for Coronaviruses. Pharmaceuticals (Basel). 2020; Mar 21. |
Emetine, Ipecac, Ipecac Alkaloids and Analogues as Potential Antiviral Agents for Coronaviruses |
Yes |
Review |
|
33 |
Arshad Ali S, Baloch M, Ahmed N, Arshad Ali A, Iqbal A. The outbreak of Coronavirus Disease 2019 (COVID-19)-An emerging global health threat. J Infect Public Health. 2020;13:644-6. |
The outbreak of Coronavirus Disease 2019 (COVID-19)-An emerging global health threat |
Yes |
No details on LPV/r therapeutics |
|
34 |
Cai Q, Huang D, Yu H, Zhu Z, Xia Z, Su Y, et al. COVID-19: Abnormal liver function tests. J Hepatol. 2020. Apr 13. |
COVID-19: Abnormal liver function tests |
Yes |
No details on LPV/r therapeutics |
|
35 |
Chan KW, Wong VT, Tang SCW. COVID-19: An Update on the Epidemiological, Clinical, Preventive and Therapeutic Evidence and Guidelines of Integrative Chinese-Western Medicine for the Management of 2019 Novel Coronavirus Disease. Am J Chin Med. 2020. Mar 13. |
Update on the Epidemiological, Clinical, Preventive and Therapeutic Evidence and Guidelines of Integrative Chinese-Western Medicine for the Management of 2019 Novel Coronavirus Disease |
Yes |
Review |
|
36 |
Scavone C, Brusco S, Bertini M, Sportiello L, Rafaniello C, Zoccoli A, et al. Current pharmacological treatments for COVID-19: what’s next? Br J Pharmacol. 2020.Apr 24. |
Current pharmacological treatments for COVID-19: what’s next? |
Yes |
Review |
|
37 |
Tursen U, Tursen B, Lotti T. Cutaneous Side-Effects of the Potential Covid-19 Drugs. Dermatol Ther. 2020. May 5. |
Cutaneous Side-Effects of the Potential Covid-19 Drugs |
Yes |
Review |
|
38 |
Testa S, Prandoni P, Paoletti O, Morandini R, Tala M, Dellanoce C, et al. Direct oral anticoagulant plasma levels’ striking increase in severe COVID-19 respiratory syndrome patients treated with antiviral agents: The Cremona experience. J Thromb Haemost. 2020. Apr 23. |
Direct oral anticoagulant plasma levels’ striking increase in severe COVID-19 respiratory syndrome patients treated with antiviral |
Yes |
No details on LPV/r therapeutics |
|
39 |
Wu F, Zhang W, Zhang L, Wang D, Wan Y. Discontinuation of antiviral drugs may be the reason for recovered COVID-19 patients testing positive again. Br J Hosp Med (Lond). 2020;81:1-2. |
Discontinuation of antiviral drugs may be the reason for recovered COVID-19 patients testing positive again |
Yes |
No details on LPV/r therapeutics |
|
40 |
Zheng XW, Tao G, Zhang YW, Yang GN, Huang P. [Drug interaction monitoring of lopinavir / ritonavir in COVID-19 patients with cancer]. Zhonghua Nei Ke Za Zhi. 2020;59:E004. |
[Drug interaction monitoring of lopinavir / ritonavir in COVID-19 patients with cancer] |
Yes |
Review |
|
41 |
Lu H. Drug treatment options for the 2019-new coronavirus (2019-nCoV). Biosci Trends. 2020;14:69-71. |
Drug treatment options for the 2019-new coronavirus (2019-nCoV) |
Yes |
Review |
|
42 |
Holzhauser L, Lourenco L, Sarswat N, Kim G, Chung B, Nguyen AB. Early Experience of COVID-19 in Two Heart Transplant Recipients: Case Reports and Review of Treatment Options. Am J Transplant. 2020. May 7. |
Early Experience of COVID-19 in Two Heart Transplant Recipients: Case Reports and Review of Treatment Options |
Yes |
Review |
|
43 |
Diurno F, Numis FG, Porta G, Cirillo F, Maddaluno S, Ragozzino A, et al. Eculizumab treatment in patients with COVID-19: preliminary results from real life ASL Napoli 2 Nord experience. Eur Rev Med Pharmacol Sci. 2020;24:4040-7. |
Eculizumab treatment in patients with COVID-19: preliminary results from real life ASL Napoli 2 Nord experience |
Yes |
No details on LPV/r therapeutics |
|
44 |
Zhong H, Wang Y, Zhang ZL, Liu YX, Le KJ, Cui M, et al. Efficacy and safety of current therapeutic options for COVID-19 – lessons to be learnt from SARS and MERS epidemic: A systematic review and meta-analysis. Pharmacol Res. 2020. Apr 30. |
Efficacy and safety of current therapeutic options for COVID-19 – lessons to be learnt from SARS and MERS epidemic: A systematic review and meta-analysis |
Yes |
Review |
|
45 |
Zhu S, Guo X, Geary K, Zhang D. Emerging Therapeutic Strategies for COVID-19 patients. Discoveries (Craiova). 2020;8:e105. |
Emerging Therapeutic Strategies for COVID-19 patients. |
Yes |
Review |
|
46 |
Cai Q, Yang M, Liu D, Chen J, Shu D, Xia J, et al. Experimental Treatment with Favipiravir for COVID-19: An Open-Label Control Study. Engineering (Beijing). 2020. Mar 18. |
Experimental Treatment with Favipiravir for COVID-19: An Open-Label Control Study |
Yes |
No details on LPV/r therapeutics |
|
47 |
Wang J. Fast Identification of Possible Drug Treatment of Coronavirus Disease-19 (COVID-19) through Computational Drug Repurposing Study. J Chem Inf Model. 2020. May 4. |
Fast Identification of Possible Drug Treatment of Coronavirus Disease-19 (COVID-19) through Computational Drug Repurposing Study |
Yes |
No details on LPV/r therapeutics |
|
48 |
Du YX, Chen XP. Favipiravir: Pharmacokinetics and Concerns About Clinical Trials for 2019-nCoV Infection. Clin Pharmacol Ther. 2020. Apr 4. |
Favipiravir: Pharmacokinetics and Concerns About Clinical Trials for 2019-nCoV Infection |
Yes |
Review |
|
49 |
Mullard A. Flooded by the torrent: the COVID-19 drug pipeline. Lancet. 2020;395:1245-6. |
Flooded by the torrent: the COVID-19 drug pipeline |
Yes |
Review |
|
50 |
Sapp JL, Alqarawi W, MacIntyre CJ, Tadros R, Steinberg C, Roberts JD, et al. Guidance on Minimizing Risk of Drug-Induced Ventricular Arrhythmia During Treatment of COVID-19: A Statement from the Canadian Heart Rhythm Society. Can J Cardiol. 2020. Apr 8. |
Guidance on Minimizing Risk of Drug-Induced Ventricular Arrhythmia During Treatment of COVID-19: A Statement from the Canadian Heart Rhythm Society |
Yes |
Guidelines |
|
51 |
Sun J, Deng X, Chen X, Huang J, Huang S, Li Y, et al. Incidence of Adverse Drug Reactions in COVID-19 patients in China: an active monitoring study by Hospital Pharmacovigilance System. Clin Pharmacol Ther. 2020. Apr 23. |
Incidence of Adverse Drug Reactions in COVID-19 patients in China: an active monitoring study by Hospital Pharmacovigilance System |
Yes |
Review |
|
52 |
Paital B, Das K, Parida SK. Inter nation social lockdown versus medical care against COVID-19, a mild environmental insight with special reference to India. Sci Total Environ. 2020;728:138914. |
Inter nation social lockdown versus medical care against COVID-19, a mild environmental insight with special reference to India |
Yes |
No details on LPV/r therapeutics |
|
53 |
Kim JY. Letter to the Editor: Case of the Index Patient Who Caused Tertiary Transmission of Coronavirus Disease 2019 in Korea: the Application of Lopinavir/Ritonavir for the Treatment of COVID-19 Pneumonia Monitored by Quantitative RT-PCR. J Korean Med Sci. 2020;35:e88. |
Letter to the Editor: Case of the Index Patient Who Caused Tertiary Transmission of Coronavirus Disease 2019 in Korea: the Application of Lopinavir/Ritonavir for the Treatment of COVID-19 Pneumonia Monitored by Quantitative RT-PCR |
Yes |
Review |
|
54 |
Rubel AR, Chong PL, Abdullah MS, Asli R, Momin RN, Mani BI, et al. Letter to the Editor: Lipemic serum in patients with COVID-19 undergoing treatment. J Med Virol. 2020. Apr 28. |
Letter to the Editor: Lipemic serum in patients with COVID-19 undergoing treatment |
Yes |
No details on LPV/r therapeutics |
|
55 |
Stower H. Lopinavir-ritonavir in severe COVID-19. Nat Med. 2020;26:465. |
Lopinavir-ritonavir in severe COVID-19 |
Yes |
No details on LPV/r therapeutics |
|
56 |
Bhatnagar T, Murhekar MV, Soneja M, Gupta N, Giri S, Wig N, et al. Lopinavir/ritonavir combination therapy amongst symptomatic coronavirus disease 2019 patients in India: Protocol for restricted public health emergency use. Indian J Med Res. 2020;151:184-9. |
Lopinavir/ritonavir combination therapy amongst symptomatic coronavirus disease 2019 patients in India: Protocol for restricted public health emergency use |
Yes |
No details on LPV/r therapeutics |
|
57 |
Docea AO, Tsatsakis A, Albulescu D, Cristea O, Zlatian O, Vinceti M, et al. A new threat from an old enemy: Reemergence of coronavirus (Review). Int J Mol Med. 2020;45:1631-43. |
A new threat from an old enemy: Reemergence of coronavirus (Review) |
Yes |
Review |
|
58 |
Dong L, Hu S, Gao J. Discovering drugs to treat coronavirus disease 2019 (COVID-19). Drug Discov Ther. 2020;14:58-60. |
Discovering drugs to treat coronavirus disease 2019 (COVID-19) |
Yes |
Review |
|
59 |
Xu K, Cai H, Shen Y, Ni Q, Chen Y, Hu S, et al. [Management of corona virus disease-19 (COVID-19): the Zhejiang experience]. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2020;49:0. |
[Management of corona virus disease-19 (COVID-19): the Zhejiang experience] |
Yes |
Review |
|
60 |
Lenkens M, de Wit H, Danser AH, Esselink AC, Horikx A, Ten Oever J, et al. [Medication and comedication in COVID-19 patients]. Ned Tijdschr Geneeskd. 2020;164. |
[Medication and comedication in COVID-19 patients]. |
Yes |
Review |
|
61 |
Zhang P, Cai Z, Wu W, Peng L, Li Y, Chen C, et al. The novel coronavirus (COVID-19) pneumonia with negative detection of viral ribonucleic acid from nasopharyngeal swabs: a case report. BMC Infect Dis. 2020;20:317. |
The novel coronavirus (COVID-19) pneumonia with negative detection of viral ribonucleic acid from nasopharyngeal swabs: a case report |
Yes |
No details on LPV/r therapeutics |
|
62 |
Plusa T. [Options for controlling new Corona virus infection – 2019-nCoV]. Pol Merkur Lekarski. 2020;48:112-9. |
[Options for controlling new Corona virus infection – 2019-nCoV] |
Yes |
Review |
|
63 |
Pavone P, Ceccarelli M, Taibi R, La Rocca G, Nunnari G. Outbreak of COVID-19 infection in children: fear and serenity. Eur Rev Med Pharmacol Sci. 2020;24:4572-5. |
Outbreak of COVID-19 infection in children: fear and serenity |
Yes |
Review |
|
64 |
Yethindra V. Role of GS-5734 (Remdesivir) in inhibiting SARS-CoV and MERS-CoV: The expected role of GS-5734 (Remdesivir) in COVID-19 (2019-nCoV)-VYTR hypothesis. International Journal of Research in Pharmaceutical Sciences. 2020 Mar 6;11:1-6. |
Role of GS-5734 (Remdesivir) in inhibiting SARS-CoV and MERS-CoV: The expected role of GS-5734 (Remdesivir) in COVID-19 (2019-nCoV)-VYTR hypothesis |
Yes |
No details on LPV/r therapeutics |
|
65 |
Md Insiat Islam R. Current Drugs with Potential for Treatment of COVID-19: A Literature Review. J Pharm Pharm Sci. 2020;23:58-64. |
Current Drugs with Potential for Treatment of COVID-19: A Literature Review |
Yes |
Review |
|
66 |
Pant S, Singh M, Ravichandiran V, Murty USN, Srivastava HK. Peptide-like and small-molecule inhibitors against Covid-19. J Biomol Struct Dyn. 2020. May 6. |
Peptide-like and small-molecule inhibitors against Covid-19 |
Yes |
No details on LPV/r therapeutics |
|
67 |
Gupta R, Ghosh A, Singh AK, Misra A. Clinical considerations for patients with diabetes in times of COVID-19 epidemic. Diabetes Metab Syndr. 2020;14:211-2. |
Clinical considerations for patients with diabetes in times of COVID-19 epidemic |
Yes |
No details on LPV/r therapeutics |
|
68 |
Wei J, Xu H, Xiong J, Shen Q, Fan B, Ye C, et al. 2019 Novel Coronavirus (COVID-19) Pneumonia: Serial Computed Tomography Findings. Korean J Radiol. 2020;21:501-4. |
2019 Novel Coronavirus (COVID-19) Pneumonia: Serial Computed Tomography Findings |
Yes |
No details on LPV/r therapeutics |
|
69 |
Li H, Wang YM, Xu JY, Cao B. [Potential antiviral therapeutics for 2019 Novel Coronavirus]. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43:170-2. |
[Potential antiviral therapeutics for 2019 Novel Coronavirus] |
Yes |
Review |
|
70 |
Gyebi GA, Ogunro OB, Adegunloye AP, Ogunyemi OM, Afolabi SO. Potential Inhibitors of Coronavirus 3-Chymotrypsin-Like Protease (3CL(pro)): An in silico screening of Alkaloids and Terpenoids from African medicinal plants. J Biomol Struct Dyn. 2020. May 5. |
Potential Inhibitors of Coronavirus 3-Chymotrypsin-Like Protease (3CL(pro)): An in silico screening of Alkaloids and Terpenoids from African medicinal plants |
Yes |
No details on LPV/r therapeutics |
|
71 |
Lu CC, Chen MY, Chang YL. Potential therapeutic agents against COVID-19: What we know so far. J Chin Med Assoc. 2020. Apr 1. |
Potential therapeutic agents against COVID-19: What we know so far |
Yes |
Review |
|
72 |
Beck BR, Shin B, Choi Y, Park S, Kang K. Predicting commercially available antiviral drugs that may act on the novel coronavirus (SARS-CoV-2) through a drug-target interaction deep learning model. Comput Struct Biotechnol J. 2020;18:784-90. |
Predicting commercially available antiviral drugs that may act on the novel coronavirus (SARS-CoV-2) through a drug-target interaction deep learning model |
Yes |
No details on LPV/r therapeutics |
|
73 |
Gentile D, Patamia V, Scala A, Sciortino MT, Piperno A, Rescifina A. Putative Inhibitors of SARS-CoV-2 Main Protease from A Library of Marine Natural Products: A Virtual Screening and Molecular Modeling Study. Mar Drugs. 2020. Apr 23. |
Inhibitors of SARS-CoV-2 Main Protease from A Library of Marine Natural Products: A Virtual Screening and Molecular Modeling Study |
Yes |
No details on LPV/r therapeutics |
|
74 |
Zhang Y, Xu J, Li H, Cao B. A Novel Coronavirus (COVID-19) Outbreak: A Call for Action. Chest. 2020;157:e99-e101. |
A Novel Coronavirus (COVID-19) Outbreak: A Call for Action |
Yes |
Review |
|
75 |
Kupferschmidt K, Cohen J. Race to find COVID-19 treatments accelerates. Science. 2020;367:1412-3. |
Race to find COVID-19 treatments accelerates |
Yes |
Review |
|
76 |
Choy KT, Wong AY, Kaewpreedee P, Sia SF, Chen D, Hui KPY, et al. Remdesivir, lopinavir, emetine, and homoharringtonine inhibit SARS-CoV-2 replication in vitro. Antiviral Res. 2020;178:104786. |
Remdesivir, lopinavir, emetine, and homoharringtonine inhibit SARS-CoV-2 replication in vitro |
Yes |
No details on LPV/r therapeutics |
|
77 |
Kumar S, Zhi K, Mukherji A, Gerth K. Repurposing Antiviral Protease Inhibitors Using Extracellular Vesicles for Potential Therapy of COVID-19. Viruses. 2020. Apr 26. |
Repurposing Antiviral Protease Inhibitors Using Extracellular Vesicles for Potential Therapy of COVID-19 |
Yes |
Review |
|
78 |
Misra DP, Agarwal V, Gasparyan AY, Zimba O. Rheumatologists’ perspective on coronavirus disease 19 (COVID-19) and potential therapeutic targets. Clin Rheumatol. 2020. Apr 10. |
Rheumatologists’ perspective on coronavirus disease 19 (COVID-19) and potential therapeutic targets |
Yes |
Review |
|
79 |
Xu X, Ong YK, Wang Y. Role of adjunctive treatment strategies in COVID-19 and a review of international and national clinical guidelines. Mil Med Res. 2020;7:22. |
Role of adjunctive treatment strategies in COVID-19 and a review of international and national clinical guidelines |
Yes |
Review |
|
80 |
Costanzo M, De Giglio MAR, Roviello GN. SARS-CoV-2: Recent Reports on Antiviral Therapies Based on Lopinavir/Ritonavir, Darunavir/Umifenovir, Hydroxychloroquine, Remdesivir, Favipiravir and Other Drugs for the Treatment of the New Coronavirus. Curr Med Chem. 2020. Apr 16 |
SARS-CoV-2: Recent Reports on Antiviral Therapies Based on Lopinavir/Ritonavir, Darunavir/Umifenovir, Hydroxychloroquine, Remdesivir, Favipiravir and Other Drugs for the Treatment of the New Coronavirus |
Yes |
Review |
|
81 |
Meziyerh S, Zwart TC, van Etten RW, Janson JA, van Gelder T, Alwayn IPJ, et al. Severe COVID-19 in a renal transplant recipient: A focus on pharmacokinetics. Am J Transplant. 2020. Apr 26. |
Severe COVID-19 in a renal transplant recipient: A focus on pharmacokinetics |
Yes |
No details on LPV/r therapeutics |
|
82 |
Nham E, Ko JH, Jeong BH, Huh K, Cho SY, Kang CI, et al. Severe Thrombocytopenia in a Patient with COVID-19. Infect Chemother. 2020. |
Severe Thrombocytopenia in a Patient with COVID-19 |
Yes |
No details on LPV/r therapeutics |
|
83 |
Unknown Author. Some drugs for COVID-19. Med Lett Drugs Ther. 2020;62:49-50. |
Some drugs for COVID-19 |
Yes |
Review |
|
84 |
Nakamura K, Hikone M, Shimizu H, Kuwahara Y, Tanabe M, Kobayashi M, et al. A sporadic COVID-19 pneumonia treated with extracorporeal membrane oxygenation in Tokyo, Japan: A case report. J Infect Chemother. 2020. Apr 18. |
A sporadic COVID-19 pneumonia treated with extracorporeal membrane oxygenation in Tokyo, Japan: A case report |
Yes |
No details on LPV/r therapeutics |
|
85 |
Yao TT, Qian JD, Zhu WY, Wang Y, Wang GQ. A systematic review of lopinavir therapy for SARS coronavirus and MERS coronavirus-A possible reference for coronavirus disease-19 treatment option. J Med Virol. 2020. Feb 27. |
A systematic review of lopinavir therapy for SARS coronavirus and MERS coronavirus-A possible reference for coronavirus disease-19 treatment option |
Yes |
Review |
|
86 |
Ford N, Vitoria M, Rangaraj A, Norris SL, Calmy A, Doherty M. Systematic review of the efficacy and safety of antiretroviral drugs against SARS, MERS or COVID-19: initial assessment. J Int AIDS Soc. 2020;23:e25489. |
Systematic review of the efficacy and safety of antiretroviral drugs against SARS, MERS or COVID-19: initial assessment |
Yes |
Review |
|
87 |
Baron SA, Devaux C, Colson P, Raoult D, Rolain JM. Teicoplanin: an alternative drug for the treatment of COVID-19? Int J Antimicrob Agents. 2020;55:105944. |
Teicoplanin: an alternative drug for the treatment of COVID-19? |
Yes |
Review |
|
88 |
Bartiromo M, Borchi B, Botta A, Bagala A, Lugli G, Tilli M, et al. Threatening drug-drug interaction in a kidney transplant patient with Coronavirus Disease 2019 (COVID-19). Transpl Infect Dis. 2020. Apr 12. |
Threatening drug-drug interaction in a kidney transplant patient with Coronavirus Disease 2019 |
Yes |
No details on LPV/r therapeutics |
|
89 |
Zhang H, Xie C, Huang Y. Treatment and Outcome of a Patient With Lung Cancer Infected With Severe Acute Respiratory Syndrome Coronavirus-2. J Thorac Oncol. 2020;15:e63-e4. |
Treatment and Outcome of a Patient With Lung Cancer Infected With Severe Acute Respiratory Syndrome Coronavirus-2 |
Yes |
No details on LPV/r therapeutics |
|
90 |
Jean SS, Lee PI, Hsueh PR. Treatment options for COVID-19: The reality and challenges. J Microbiol Immunol Infect. 2020. Apr 4. |
Treatment options for COVID-19: The reality and challenges |
Yes |
Review |
|
91 |
Stebbing J, Phelan A, Griffin I, Tucker C, Oechsle O, Smith D, et al. COVID-19: combining antiviral and anti-inflammatory treatments. Lancet Infect Dis. 2020;20:400-2. |
COVID-19: combining antiviral and anti-inflammatory treatments |
Yes |
No details on LPV/r therapeutics |
|
92 |
Carmona-Bayonas A, Jimenez-Fonseca P, Castanon E. A Trial of Lopinavir-Ritonavir in Covid-19. N Engl J Med. 2020. May 5 |
A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19 |
Yes |
Letter to the editor |
|
93 |
Corrao S, Natoli G, Cacopardo B. A Trial of Lopinavir-Ritonavir in Covid-19. N Engl J Med. 2020. May 5. |
A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19 |
Yes |
Letter to the editor |
|
94 |
Dalerba P, Levin B, Thompson JL. A Trial of Lopinavir-Ritonavir in Covid-19. N Engl J Med. 2020. May 5. |
A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19 |
Yes |
Letter to the editor |
|
95 |
Havlichek D, Jr. A Trial of Lopinavir-Ritonavir in Covid-19. N Engl J Med. 2020. May 5. |
A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19 |
Yes |
Letter to the editor |
|
96 |
Kunz KM. A Trial of Lopinavir-Ritonavir in Covid-19. N Engl J Med. 2020. May 5. |
A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19 |
Yes |
Letter to the editor |
|
97 |
Shah B, Modi P, Sagar SR. In silico studies on therapeutic agents for COVID-19: Drug repurposing approach. Life Sci. 2020;252:117652. |
In silico studies on therapeutic agents for COVID-19: Drug repurposing approach |
Yes |
No details on LPV/r therapeutics |
|
98 |
Kim Y, Kwon O, Paek JH, Park WY, Jin K, Hyun M, et al. Two distinct cases with COVID-19 in kidney transplant recipients. Am J Transplant. 2020. Apr 26. |
Two distinct cases with COVID-19 in kidney transplant recipients |
Yes |
|
|
99 |
Qiu L, Jiao R, Zhang A, Chen X, Ning Q, Fang F, et al. A Typical Case of Critically Ill Infant of Coronavirus Disease 2019 With Persistent Reduction of T Lymphocytes. Pediatr Infect Dis J. 2020. May 1. |
A Typical Case of Critically Ill Infant of Coronavirus Disease 2019 With Persistent Reduction of T Lymphocytes |
Yes |
No details on LPV/r therapeutics |
|
100 |
Giudicessi JR, Noseworthy PA, Friedman PA, Ackerman MJ. Urgent Guidance for Navigating and Circumventing the QTc-Prolonging and Torsadogenic Potential of Possible Pharmacotherapies for Coronavirus Disease 19 (COVID-19). Mayo Clin Proc. 2020. Apr 7. |
Urgent Guidance for Navigating and Circumventing the QTc-Prolonging and Torsadogenic Potential of Possible Pharmacotherapies for Coronavirus Disease 19 (COVID-19) |
Yes |
No details on LPV/r therapeutics |
|
101 |
Taniguchi H, Ogawa F, Honzawa H, Yamaguchi K, Niida S, Shinohara M, et al. Veno-venous extracorporeal membrane oxygenation for severe pneumonia: COVID-19 case in Japan. Acute Med Surg. 2020;7:e509. |
Veno-venous extracorporeal membrane oxygenation for severe pneumonia: COVID-19 case in Japan |
Yes |
No details on LPV/r therapeutics |
|
102 |
Larreal Y. Pandemic of the new coronavirus SARSCoV-2 in Venezuela. [Spanish]. Investigacion Clinica (Venezuela). 2020;61:pp 1-3. |
Pandemic of the new coronavirus SARSCoV-2 in Venezuela. |
Yes |
No details on LPV/r therapeutics |
|
103 |
Nutho B, Mahalapbutr P, Hengphasatporn K, Pattaranggoon NC, Simanon N, Shigeta Y, et al. Why Are Lopinavir and Ritonavir Effective against the Newly Emerged Coronavirus 2019? Atomistic Insights into the Inhibitory Mechanisms. Biochemistry. 2020. Apr 24. |
Why Are Lopinavir and Ritonavir Effective against the Newly Emerged Coronavirus 2019? Atomistic Insights into the Inhibitory Mechanisms |
Yes |
Review |
|
104 |
Ning L, Liu L, Li W, Liu H, Wang J, Yao Z, et al. Novel coronavirus (SARS-CoV-2) infection in a renal transplant recipient: Case report. Am J Transplant. 2020. Apr 10. |
Novel coronavirus (SARS-CoV-2) infection in a renal transplant recipient: Case report |
Yes |
No details on LPV/r therapeutics |
|
105 |
Decaro N, Martella V, Saif LJ, Buonavoglia C. COVID-19 from veterinary medicine and one health perspectives: What animal coronaviruses have taught us. Res Vet Sci. 2020;131:21-3. |
COVID-19 from veterinary medicine and one health perspectives: What animal coronaviruses have taught us |
Yes |
No details on LPV/r therapeutics |
|
106 |
Ortega JT, Serrano ML, Pujol FH, Rangel HR. Unrevealing sequence and structural features of novel coronavirus using in silico approaches: The main protease as molecular target. Excli j. 2020;19:400-9. |
Unrevealing sequence and structural features of novel coronavirus using in silico approaches: The main protease as molecular target |
Yes |
No details on LPV/r therapeutics |
|
107 |
Das S, Sarmah S, Lyndem S, Singha Roy A. An investigation into the identification of potential inhibitors of SARS-CoV-2 main protease using molecular docking study. J Biomol Struct Dyn. 2020. May 2. |
An investigation into the identification of potential inhibitors of SARS-CoV-2 main protease using molecular docking study |
Yes |
No details on LPV/r therapeutics |
|
108 |
Young BE, Ong SWX, Kalimuddin S, Low JG, Tan SY, Loh J, et al. Epidemiologic Features and Clinical Course of Patients Infected With SARS-CoV-2 in Singapore. Jama. 2020. Mar 3. |
Epidemiologic Features and Clinical Course of Patients Infected With SARS-CoV-2 in Singapore |
Yes |
No details on LPV/r therapeutics |
|
109 |
Alpern JD, Gertner E. Off-Label Therapies for COVID-19-Are We All In This Together? Clin Pharmacol Ther. 2020. Apr 20. |
Off-Label Therapies for COVID-19-Are We All In This Together? |
Yes |
Review |
|
110 |
Buonaguro FM, Puzanov I, Ascierto PA. Anti-IL6R role in treatment of COVID-19-related ARDS. J Transl Med. 2020;18:165. |
Anti-IL6R role in treatment of COVID-19-related ARDS |
Yes |
No details on LPV/r therapeutics |
|
111 |
Fu B, Xu X, Wei H. Why tocilizumab could be an effective treatment for severe COVID-19? J Transl Med. 2020;18:164. |
Why tocilizumab could be an effective treatment for severe COVID-19? |
Yes |
No details on LPV/r therapeutics |
|
112 |
Calligari P, Bobone S, Ricci G, Bocedi A. Molecular Investigation of SARS-CoV-2 Proteins and Their Interactions with Antiviral Drugs. Viruses. 2020; Apr 14. |
Molecular Investigation of SARS-CoV-2 Proteins and Their Interactions with Antiviral Drugs |
Yes |
No details on LPV/r therapeutics |