Abstract
Bariatric surgical procedures are being performed at an exponential rate. Gastric banding is a commonly performed Bariatric surgical procedure with band erosion being a known complication. Until recently eroded Gastric Bands have undergone surgical removal. Recent reports have described endoscopic removal using a biliary guide-wire and biliary mechanical lithotripter.
Aim: To determine the safety and feasibility of endoscopic removal of eroded gastric bands using lithotripsy devices following Bariatric surgery.
Methods: Thirteen patients (9w, 3m), age 33–59 (mean 45) presented with a diagnosis of eroded gastric band. These include 9 adjustable lap bands. Presenting symptoms included pain 10/13, N/V 7/13, fever/port infection 1/13. All patients had confirmation of gastric band erosion with endoscopy and CT scan 13/13.
Results: All patients with non-adjustable gastric bands were removed successfully, endoscopically. Of the patients with Adjustable Lap Bands, endoscopic removal was successful in 8/9 patients. The failed attempt was in a patient whose Band had significant fibrotic component and non-visualization of the buckle. This patient required laparoscopic removal. All patients underwent post-op contrast upper GI imaging to exclude gastric leak.
Conclusion: Patients with Gastric Band erosion present most often with abdominal pain, followed by nausea and vomiting. Diagnosis is established by endoscopy and CT imaging. Endoscopic removal is highly but not universally successful and requires coordination with a Bariatric Surgeon for the removal of the adjustable port and removal of the band in the setting of endoscopic failure. The endoscopist needs to familiarize him with Bariatric Surgical procedures and their inherent complications and eventually assist in their care when called upon.
Introduction
Obesity is defined as abnormal or excessive fat accumulation that presents as a risk to health [1]. Despite obesity being a well identified and acknowledged problem, it continues to grow as a global epidemic [2]. Obesity has emerged as a major problem, the primary reason being an imbalance between the consumption and expenditure of calories. Since 1975, the number of obese people has increased by three times across the globe. According to the 2016 World Health Organization statistics, 650 million people (13%) 18 years and above have been identified as obese [3]. 36.5% of the total population of United States is Obese [4]. Obese people can have a significantly negative impact on the quality of their lives in terms of an increased risk of having diabetes mellitus type 2, infertility, cardiovascular diseases, respiratory disorders, malignancies, as well as social and functional limitations [5].
Bariatric care has expanded over the period to be identified as a growing field for consideration as a treatment option for obesity [6,7]. Bariatric procedures cause weight loss by limiting the amount of food the stomach can hold or malabsorption of nutrients or a combination of both. The commonly performed bariatric procedures include Roux-en-Y Gastric Bypass, Sleeve Gastrectomy, Adjustable Gastric Band, and Biliopancreatic Diversion with Duodenal Switch [8].
In the United States, trends have been shifting towards Laparoscopic Gastric bands as means of attaining weight loss [9]. Where lap bands have proven as an effective alternative to the conventional weight loss methods, they come with a cost of complications ranging from mild to serious [10].
The pathophysiology of gastric band erosion has yet to be understood [11]. The established understanding of gastric band erosion reveals that acute and chronic tissue damage could be a potential trigger to initiate band erosion [12]. Undiagnosed gastric perforations that may occur during band placements and early infections can serve as the possible causes of early erosions. Late erosions are caused by gastric band induced high pressure leading to chronic ischemia [13,14]. This prolonged ischemia gives way to band erosion through the mucosal layer and hence a perception of pain.
Gastric band erosion has been identified as a common complication with its incidence varying from 0.23% to 32.65% [15]. Symptoms of gastric band erosion include abdominal pain, excessive vomiting, weight loss cessation or unexplained weight regain and the inability to regulate the stoma [16]. Endoscopic removal of eroded gastric bands has been identified as a potent and safe technique to address this complication [17].
We report a unique approach towards the removal of eroded gastric bands using a biliary guided wire and biliary mechanical lithotripter. This method was applied in 19 patients with eroded gastric bands and represents one of the largest case series in this respect. Literature review reveals that our technique is one of its kinds and can potentially contribute to determining the safety and feasibility of endoscopic removal of eroded gastric bands following Bariatric Surgery.
Materials and Methods
Thirteen patients (9w, 3m), age 33–59 (mean 45) presented to the University of Texas, and Memorial Hermann Hospital with symptoms leading to a diagnosis of eroded gastric lap band. This included 4 non-adjustable and 9 adjustable (attached injection port) lap bands. Presenting symptoms included; pain 10/13, nausea/vomiting 7/13, fever/port infection 1/13. Patients presented 5–24 weeks from start of symptoms (mean 16 weeks). All patients had confirmation of gastric band erosion with upper endoscopy and CT scan imaging.
Procedure technique; a flexible biliary hydrophilic guide-wire with flexible tip (0.025 in x 450cm) is advanced through the band while the endoscope is withdrawn (Figure 1). The endoscope is re-advanced alongside the wire and the distal tip is captured with forceps and withdrawn through the mouth (Figure 2). With the two ends of the wire now outside the patient’s mouth a flexible lithotripter cable, the Emergency Lithotripter System BML-110A-1 (Olympus America) (Figure 3) is advanced over the two ends of the wire until the tip rests against the gastric band (Figure 4). The lithotripter handle is then attached to the cable and progressively ratcheted down until the wire cuts across the band (Figure 5). The surgeon detaches and removes the port in those with adjustable bands while the endoscopist removes the cut band with a stiff, braided snare (Figure 6).

Figure 1. Guide-wire across the eroded lap band.

Figure 2. Guide-wire across the eroded lap band and both ends outside the mouth.
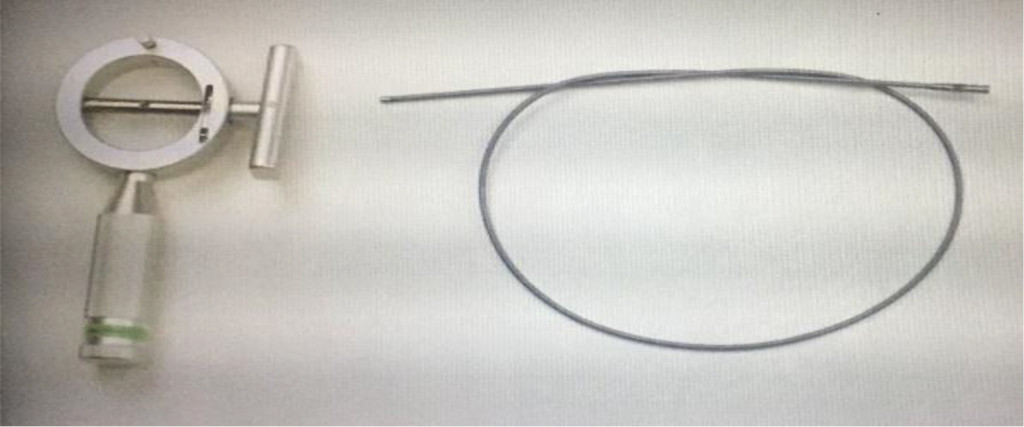
Figure 3. Emergency Lithotripter System.
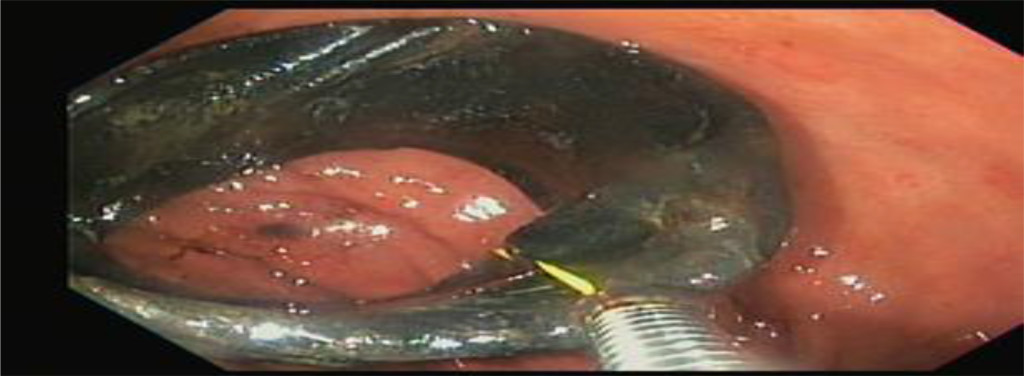
Figure 4. Lithotripter advanced through the guide-wire now rests against the eroded lap band.

Figure 5.Wire cutting across the band.

Figure 6. Removed eroded lap band.
Results
All patients with non-adjustable gastric bands were removed successfully, endoscopically using the above technique. Of the patients with Adjustable Lap Bands, endoscopic removal was successful in 8/9 patients. The failed attempt was in a patient whose Band had significant fibrotic component and non-visualization of the buckle. This patient required laparoscopic removal at the same time as port removal. Procedure time recorded ranged from 18 minutes to 32 minutes (mean 24 minutes). All patients underwent post-op contrast upper GI imaging using dilute barium to exclude gastric leak within 12 hours of band removal. No leaks or perforations were identified. Minor bleeding occurred in one patient which resolved spontaneously. Patients were discharged 1–4 days post-op (mean 1.4 days). One patient with port infection required prolonged hospitalization for IV antibiotics and fever resolution.
Discussion
Obesity has been recognized as an important contributive factor towards premature deaths [18]. Laparoscopic gastric banding has evolved as an effective strategy for weight loss that has been proven to decrease total body weight by up to 20% [19]. Where gastric bands are now recognized widely as an effective tool for weight loss and significant contributions towards comorbidities of obesity, its complications like port or tubing malfunction, band slippage, and obstruction of the stoma, band erosion, pouch dilation, and infection cannot be ignored [20].
Where a definite cause of gastric band erosion has yet to be established, it is imperative to apply certain techniques at the time of insertion of gastric band to minimize the risk of gastric band erosion [12,21]. External as well as internal pressure applied to the gastric wall has been hypothesized as a key etiologic factor of band erosion [22]. External pressure may be induced by band over-filling, band rapid filling or band infection [23,24]. Binge eating after the band placement surgery is a contributive factor towards internal pressure [25,20]. One of the important pathophysiologic causes of band erosion stems from the recognition of gastric band as a foreign body by the immune system [26–28]. This results in the formation of an encapsulating fibrotic shell around the eroded lap band that leads to tissue contraction. This shrinked tissue protects the integrity of the fistulous tract [29]. As lap band erosion through the stomach wall occurs over a period of several years, gastric perforation is a rare occurrence [30]. This pathophysiology reflects that active perforation is absent in eroded lap bands. Endoscopic removal of lap bands is therefore a safe yet effective procedure for the removal of eroded lap bands [31–36].
While patients with gastric band erosions can be completely asymptomatic, symptoms if present include repeated port infections, bowel obstruction, abdominal pain and rarely as serious as sepsis with peritonitis [37]. These being mentioned, band erosions can also lead to serious consequences like massive GI hemorrhage and circulatory collapse [38,39], pyelophlebitis of the portal vein [40] and intra-abdominal abscess [41]. Therefore, it is crucial to remove the eroded gastric band [8].
Various techniques have evolved over the course of time for the removal of eroded gastric bands. Unfortunately, literature review is lacking with respect to the comparison of different techniques used for the retrieval of eroded gastric bands [42]. However, the efficacy and design specific model of each technique varies from case to case. For instance, the hybrid technique considers the simultaneous use of laparoscopic and endoscopic methods to complement and facilitate each other [3]. Where some studies advocate the safety of removal of eroded gastric bands using a Single Incision Laparoscopic Surgery (SILS) [43], others urge on the use of standard endoscopy equipment for the removal of eroded gastric bands [44]. A study by Kohn GP explains the superiority of laparoscopic removal in terms of time duration from band erosion to band removal [45]. Nevertheless, physicians have yet to establish certain set guidelines identifying the superiority of one technique over the other in different situations. Due to the limitations of endoscopic and laparoscopic procedures in this regard, the role of a Bariatric surgeon becomes crucial. In certain cases, laparoscopic and endoscopic techniques may both fail in removing the gastric band in which case the role of bariatric surgeon emerges as one of utmost importance [46–48].
In our series band removal was successfully performed using our technique in 12/13 patients. CT scan and endoscopy was performed to confirm the diagnosis. We had 4 patients with adjustable gastric bands and 9 patients with non-adjustable gastric bands. Contrast upper Gastrointestinal imaging was performed in all patients after the procedure to exclude gastric leaks. Success rate with our technique was 92%. We had a failed attempt in a single patient. In this case the band had undergone significant fibrosis obscuring the buckle. In this patient laparoscopic removal was performed.
Conclusion
Abdominal pains followed by nausea and vomiting are the most common symptoms of gastric band erosion. CAT scan and endoscopy are used as the primary tools for establishment of a diagnosis. Bariatric surgeons and endoscopists should work in a closely coordinated team to address the complications of gastric band removal. Lithotripsy devices can be effectively and safely used in the retrieval of eroded gastric bands.
References
- World Health Organization, Health Topics. Obesity: Commission on Ending Childhood Obesity, WHO, Geneva, Switzerland.
- Nia Mitchell, Vicki Catenacci, Holly R. Wyatt, James O. Hill (2012) Obesity: Overview of An Epidemic. Psychiatr Clin North Am 34: 717–732.
- World Health Organization, News/Fact sheets/Detail/Obesity and overweight, WHO, Geneva, Switzerland.
- Centers for Disease Control and Prevention, Overweight & Obesity, Data & Statistics, U.S. Department of Health & Human Services, USA.
- Pozza C, Isidori AM (2018) What’s Behind the Obesity Epidemic. In: Laghi A, Rengo M (eds.). Imaging in Bariatric Surgery. Springer International Publishing AG, Cham, Switzerland.
- Roslin MS, Cripps C, Peristeri A (2015) Bariatric and metabolic surgery: current trends and what’s to follow. Curr Opin Gastroenterol 31: 513–518. [Crossref]
- David E Arterburn, Anita P Courcoulas (2014) Bariatric surgery for obesity and metabolic conditions in adults. BMJ 349: 3961.
- American Society for Metabolic & Bariatric Surgery, Bariatric Surgery Procedures. ASMBS, Gainesville, Florida, USA.
- Favretti F, Ashton D, Busetto L, Segato G, De Luca M (2009) The gastric band: first-choice procedure for obesity surgery. World J Surg 33: 2039–2048. [Crossref]
- Sven Gustavsson, Agneta Westling (2002) Laparoscopic Adjustable Gastric Banding: Complications and Side Effects Responsible for the Poor Long-Term Outcome. Surgical Innovation 9: 2
- Manatakis DK, Ioannis Terzis, Kyriazanos ID, Dontas ID, Stoidis CN, et al (2014) Simultaneous Gastric and Duodenal Erosions due to Adjustable Gastric Banding for Morbid Obesity. Case Reports in Surgery 146980: 4
- Chang Ik Yoon, Kyung Ho Pak, Seong Min Kim (2012) Early experience with diagnosis and management of eroded gastric bands. J Korean Surg Soc 82: 18–27. [Crossref]
- Gee Young Yun, Woo Sub Kim, Hye Jin Kim, Sun Hyung Kang, Hee Seok Moon, et al (2016) Asymptomatic Gastric Band Erosion Detected during Routine Gastroduodenoscopy. Clin Endosc 49(3): 294–297. [Crossref]
- Bernard Hainaux, Emmanuel Agneessens, Erika Rubesova, Vinciane Muls, Quentin Gaudissart, et al (2005) Intragastric Band Erosion After Laparoscopic Adjustable Gastric Banding for Morbid Obesity: Imaging Characteristics of an Underreported Complication. American Journal of Roentgenology184: 109–112.
- Mario Rodarte-Shade, Gustavo Torres Barrera, Jose H. Flores Arredondo, Roberto Rumbaut Diaz (2013) Hybrid Technique for Removal of Eroded Adjustable Gastric Band. JSLS 17: 338–341. [Crossref]
- H Joseph Naim, Piotr J Gorecki, Leslie Wise (2005) Early Lap-Band Erosion Associated With Colonic Inflammation: A Case Report and Literature Review. JSLS 9: 102–104. [Crossref]
- Spann MD, Aher CV, English WJ, Williams DB (2017) Endoscopic management of erosion after banded bariatric procedures. Surg Obes Relat Dis13: 1875–1879. [Crossref]
- Iyad Eid, Daniel W. Birch, Arya M. Sharma, Vadim Sherman, Shahzeer Karmali (2011) Complications associated with adjustable gastric banding for morbid obesity: a surgeon’s guide. Can J Surg 54: 61–66. [Crossref]
- Chieh Jack Chiu, Daniel W. Birch, XinZhe Shi, Shahzeer Karmali (2013) Outcomes of the adjustable gastric band in a publicly funded obesity program. Can J Surg 56: 233–236. [Crossref]
- Charles Kodner, Daniel R. Hartman (2014) Complications of Adjustable Gastric Banding Surgery for Obesity. Complications of Adjustable Gastric Banding Surgery for Obesity. Am Fam Physician 89: 813–818.
- Abdulzahra A. Hussain, Jacqueline Nicholls, Shamsi S. El-Hasani (2014) Laparoscopic Adjustable Gastric Band: How to Reduce the Early Morbidity. JSLS 18: 2014.00241[Crossref]
- Doğan ÜB, Akova A, Solmaz S, Aydin M (2010) Gastroscopic removal of a migrated adjustable gastric band: a case report. Turk J Gastroenterol 21: 297–301. [Crossref]
- Mittermair RP, Weiss H, Nehoda H, Aigner F (2002) Uncommon intragastric migration of the Swedish adjustable gastric band. Obes Surg 12: 372–375.[Crossref]
- Neto MP, Ramos AC, Campos JM, Murakami AH, Falcão M, et al (2010) Endoscopic removal of eroded adjustable gastric band: lessons learned after 5 years and 78 cases. Surg Obes Relat Dis 6: 423–427 [Crossref]
- Pawel Rogalski, Hady HR, Andrzej Baniukiewicz, Andrzej Dąbrowski, Fabian Kaminski, et al (2012) Gastric band migration following Laparoscopic Adjustable Gastric Banding (LAGB): two cases of endoscopic management using a gastric band cutter. Wideochir Inne Tech Maloinwazyjne 7: 114–117. [Crossref]
- Partha Hota, Dina Caroline, Sonia Gupta, Omar Agosto (2018) Laparoscopic adjustable gastric band erosion with intragastric band migration: A rare but serious complication. Radiology Case Reports 13: 76–80
- David Collado-Pacheco, Luis Ramon Rábago-Torre, Maria Arias-Rivera, Alejandro Ortega-Carbonel, Ana Olivares-Valles, et al (2016) Endoscopic extraction of adjustable gastric bands after intragastric migration as a complication of bariatric surgery: technique and advice. Endosc Int Open 4: 673–677. [Crossref]
- Giovanni D De Palma, Antonio Formato, Vincenzo Pilone, Maria Rega, Maria Elena Giuliano, et al (2006) Endoscopic management of intragastric penetrated adjustable gastric band for morbid obesity. World J Gastroenterol 12: 4098–4100. [Crossref]
- Edo Oscar Aarts, Bas van Wageningen, Frits Berends, Ignace Janssen, Peter Wahab, et al (2015) Intragastric band erosion: Experiences with gastrointestinal endoscopic removal. World J Gastroenterol 21: 1567–1572. [Crossref]
- SJW Monkhouse, JDT Morgan, SA Norton (2009) Complications of Bariatric Surgery: Presentation and Emergency Management – a Review. Ann R Coll Surg Engl 91: 280–286. [Crossref]
- Neto MP, Ramos AC, Campos JM, Murakami AH, Falcão M, et al (2010) Endoscopic removal of eroded adjustable gastric band: lessons learned after 5 years and 78 cases. Surg Obes Relat Dis 6: 423–427. [Crossref]
- Peter M. Bertin, Marc L. Costa (2012) Endoscopic Removal of Eroded Gastric Band Using Standard Endoscopy Equipment. Bariatric Times 9: 20–22
- Shehab H, Gawdat K (2017) Endoscopic Management of Eroded Bands Following Banded-Gastric Bypass (with Video). Obes Surg 27: 1804–1808. [Crossref]
- Dogan ÜB, Akin MS, Yalaki S, Akova A, Yilmaz C (2014) Endoscopic management of gastric band erosions: a 7-year series of 14 patients. Can J Surg 57: 106–111.[Crossref]
- Dogan UB, Dal MB (2015) An 8-Year Experience With Endoscopic Management of Eroded Gastric Bands. Surg Laparosc Endosc Percutan Tech 25: 140–144 [Crossref]
- Lattuada E, Zappa MA, Mozzi E, Fichera G, Granelli P, et al (2007) Band erosion following gastric banding: how to treat it. Obes Surg 17: 329–333. [Crossref]
- Gee Young Yun, Woo Sub Kim, Hye Jin Kim, Sun Hyung Kang, Hee Seok Moon, et al (2016) Asymptomatic Gastric Band Erosion Detected during Routine Gastroduodenoscopy. Clin Endosc 49: 294–297. [Crossref]
- Rao AD, Ramalingam G (2006) Exsanguinating hemorrhage following gastric erosion after laparoscopic adjustable gastric banding. Obes Surg 16: 1675–1678. [Crossref]
- Campos J, Ramos A, Galvão Neto M, Siqueira L, Evangelista LF, et al (2007) Hypovolemic shock due to intragastric migration of an adjustable gastric band. Obes Surg 17: 562–564. [Crossref]
- De Roover A, Detry O, Coimbra C, Hamoir E, Honoré P, Meurisse M. (2006) Pylephlebitis of the portal vein complicating intragastric migration of an adjustable gastric band. Obes Surg 16: 369–71. [Crossref]
- Wylezol M, Sitkiewicz T, Gluck M, Zubik R, Pardela M (2006) Intra-abdominal abscess in the course of intragastric migration of an adjustable gastric band: a potentially life-threatening complication. Obes Surg 16: 102–104. [Crossref]
- Ümit Bilge Dogan, Mustafa Salih Akin, SerkanYalaki, Atilla Akova, CengizYilmaz (2014) Endoscopic management of gastric band erosions: a 7-year series of 14 patients. Can J Surg 57: 2
- Spitali, K. De Vogelaere, G. Delvaux (2013) Removal of Eroded Gastric Bands Using a Transgastric SILS Device. Case Reports in Surgery 2013: 852747.
- Peter M. Bertin and Marc L. Costa (2012) Endoscopic Removal of Eroded Gastric Band Using Standard Endoscopy Equipment Bariatric Times 9: 20–22
- Kohn GP, Hansen CA, Gilhome RW, McHenry RC, Spilias DC, Hensman C (2012) Laparoscopic management of gastric band erosions: a 10-year series of 49 cases. Surg Endosc 26: 541–545. [Crossref]
- Basa NR, Dutson E, Lewis C, Derezin M, Han S, Mehran A (2008) Laparoscopic transgastric removal of eroded adjustable band: a novel approach. Surg Obes Relat Dis 4: 194–197 [Crossref]
- Denis JoséEchaverry-Navarrete, Angélica Maldonado-Vázquez, PabloCortes-Romano, RicardoCabrera-Jardines, Erwin EduardoMondragón-Pinzón, et al (2015) Gastric band erosion: Alternative management. Cirugía y Cirujanos 83: 418–423
- Ashvini Abeysekera, Jerry Lee, Simon Ghosh, Craig Hacking (2017) Migration of eroded laparoscopic adjustable gastric band causing small bowel obstruction and perforation. BMJ 2017: 2017–219954.